
Ahmad Barotchi
@ABarotchi1
Followers
1,447
Following
1,974
Media
67
Statuses
34,072
Radiology SpR. Prefer to retweet as I save my witty writing for imaging reports. Views are my own. Retweet does not necessarily mean endorsement (but may do).
Yorkshire and The Humber, Engl
Joined December 2022
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
BAMBAM
• 256932 Tweets
#BLEACH
• 195503 Tweets
Pete Rose
• 165498 Tweets
PlayStation
• 151283 Tweets
JO1 WHERE DO WE GO
• 77068 Tweets
Happy New Month
• 67027 Tweets
Jimmy Carter
• 61784 Tweets
#ไฟไหม้รถบัส
• 61397 Tweets
#LINEマンガガチャ
• 55817 Tweets
Goff
• 38243 Tweets
सोनम वांगचुक
• 37242 Tweets
Independence Day
• 29538 Tweets
コーヒーの日
• 26248 Tweets
都民の日
• 19931 Tweets
KerjaJOKOWI PRABOWOlanjutkan
• 16227 Tweets
YukBARENG MajukanBANGSA
• 15539 Tweets
Pancasila
• 13287 Tweets
世界4位
• 10870 Tweets
夕刊フジ
• 10229 Tweets


















To all doctors feeling distraught about today's legislation, don't.
This was inevitable.
They still need our cooperation. And royal colleges which we are slowly reclaiming. The chess pieces are falling all around them and this is just a sign of desperation. Make no mistake

Extremely disappointing that Peers have tonight waved through legislation that will blur the lines between PAs and doctors, with potentially dangerous consequences for patients.
We thank Peers who urged Government to heed the warnings of the medical profession.
68
835
2K
14
144
538
This is how we've been hoodwinked.
They will quote 20%.
As if the last 2 years of inflation didn't exist.
Reality is this is just over 6% out of the 35% restoration to previous pay we've been asking for (IT'S NOT A RAISE)
It's a no from me

@DrDMcGregor
It’s not 20% out of 35%. Because it includes old pay rise and the inflation since this started stands at 15.75%. So you’re about 6% above inflation maximum.
You’re at 6% out of 35%.
7
37
187
4
55
288
This individual is likely great at her job, but the title "trainee consultant" is absurd. Consultant in hospital to most patients means one thing.
To double down, Rotherham trust have hilariously disabled comments instead of addressing the absurdity they were critiquing
20
52
270
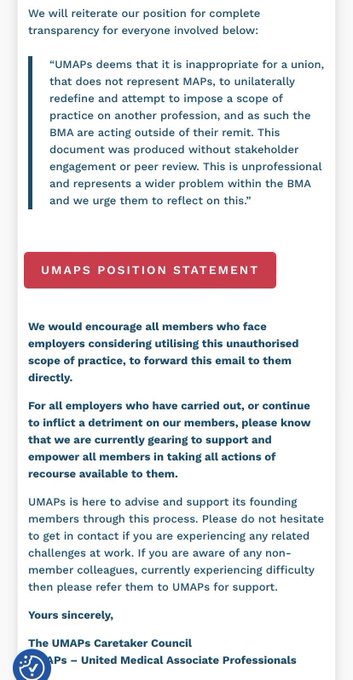
Deplorable behaviour from the unprofessional PA scam org pretending to be a union.
The scope is to protect Drs & patients, and they're worried they won't be able to cosplay to the detriment of patient wellbeing

The PA “union” is preparing to take action against NHS trusts and GP partners who try to limit PA scope of practice.
They don’t give a shit about patients or medicine, only their own self-aggrandisement.
Credit to
@medicalmodelbri
49
99
483
14
52
210
People need to think about just how sinister this is.
Someone is looking to collect outcome data for children managed by non doctors at a hospital.
That means comparing data on admissions, readmissions ,hospital stays, and adverse outcomes. Among other things
1/2


1
54
199
@StGeorgesUni
If you have Drs, nurses, physios, dentists, all graduating together, this wouldn't have had so much attention.
To do this at a time when there is a politically driven conflation between Drs & PAs suggests you are being disingenuous. You can't be that blind - this is intentional
0
17
197
PA doing A-V fistula formations. Worried about current scrutiny - so holds off them a little...
Why? Did they realise they weren't adequately trained for it?
No. In case they mess up and it makes them & other PAs look bad.
It seems public relations/image > patient safety
@ExplosiveEnema2
@UMAPsUK
“I hesitated just in case something went wrong and he would use it against me and PAs?”
That’s utterly horrifying.
Where are PA courses finding these people?
9
20
130
6
43
191
There's simething quite obvious here which needs to be said, and supporters of the government's workforce plan need to come to terms with.
When this is the behaviour of people who are courted by the DHSC and GMC, do their promoters not wonder:
"Are we the bad guys?"
1/n

I have been subjected to immense stress and threats to my livelihood due to vexatious police & GMC referrals by Mr Nash, the leader of a PA union-in-waiting, all of which have thankfully been dismissed. He has faced no consequences, leaving me anxious about what he might do next.
23
224
637
3
50
178
Outstanding guidance from the BMA, and fair.
You must question the motives of those who disagree with this.
Now that a group democratically representing doctors has consulted with various specialties, that is all we need. Nothing as comprehensive has come out thus far
"Patients must know who is treating them and the skills and abilities that clinician has."
Today, we have published new guidance on the scope of responsibilities for Medical Associate Professionals (MAPs).
Read more here:
61
453
1K
4
33
166
@jkcyriac23
@gmcuk
You have an issue with the truth and so you tag the regulator.
You aren't equivalent even to a 4th year medical student in terms of educational rigour, training and selective course admission.
If the truth upsets you, that doesn't make it inherently unkind
4
2
159
Often, when people talk about "modernising" nhs workforce/staffing, it means one thing:
Diluting standards. Replacing doctors and nurses with people who are less qualified.
Remember this

'They are there to work alongside doctors not instead of doctors.'
Health Secretary Victoria Atkins reiterates 'regulations' on physician associates after the death of 30-year-old Emily Chesterton.
178
136
354
1
46
155
This. This is what IR needs.
An asset for the future of radiology, something to help lists & workflows, to develop IR more like a specialty. I hear Hull have done similar.
Dr Gupta deserves full praise. Other quote tweets echo my sentiments.
IR consultants, take note

@Gastrografin1
@marklittle_IR
@RBNHSFT
@nhsuhcw
We've had an IR FY2
@nhsuhcw
for 4yrs.
Takes 1month to train them, then an amazing asset for 3months.
I understand benefit of PA, as only need to be trained once.
However about 30% of my FY2s have entered radiology training to become potential future IR Consultant colleagues!
23
75
382
4
21
142
The GMC is standing against the very experts it is supposed to regulate, ignoring the concerns of experts about regulation and professional standards.
To add further humiliation to them, they've also just been community noted on twitter.
It's quite glorious

Today we have responded to the BMA, strongly rejecting the basis on which they have proposed to bring legal proceedings.
You can read our statement on our website -
236
55
127
3
33
140
Can i contextualise just how fucked this is for you all...
Heading a major trauma centre comes with certain prestige and funding.
Rather than confess they can't manage major traumas with this woeful staffing, trust has ploughed on to avoid admitting as much
1/2
KCH should now issue a statement saying they are no longer an MTC as the service is unsafe.
The Very Senior Managers should resign as they are being asked to do the impossible.
They won’t, because they are prioritising their own careers over the lives of patients (1/2)
2
30
170
2
33
137
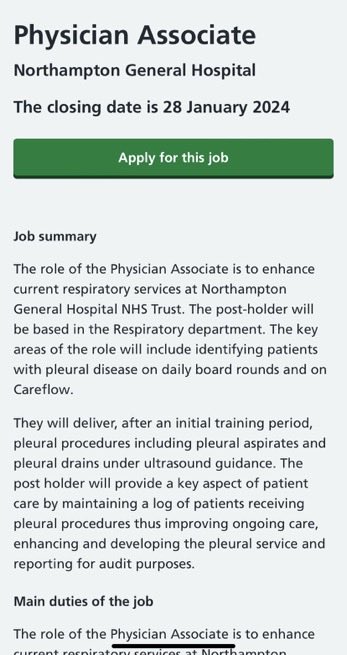
If you are the consultant who has signed off on this monstrosity of inappropriate scope, you need to have a good, long look in the mirror

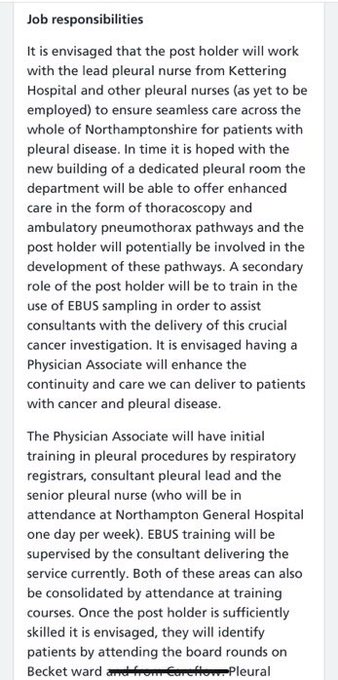
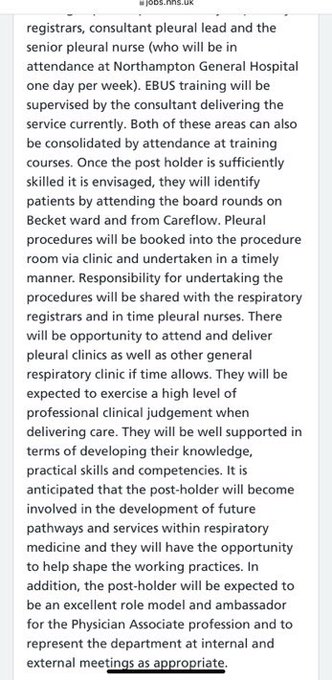
Northampton
#Respiratory
Patients
#PhysicianAssociates
#Pleural
Procedures
#EBUS
Job Description ⬇️
Risks ?
@BTSrespiratory
@EuroRespSoc
@NHSEnglandNMD
@NGHnhstrust
@TheBMA
@doctor_oxford
@TheLancet
@TheLawyermag
@LBC
16
18
54
4
43
134
Hi all,
Some of you may be aware I'm running for the RCR Specialty Training Board this year. It's a council position - a chance to see how things work, and to promote pro-radiologist policies to maintain standards & help trainees
10
38
127
This gets shadier by the day.
And GMC want to act as though their hand has been forced.
Charlie Massey has to leave, he's obviously had the poisonous influence people warned about when he was appointed, with the political connections to get his way

All credit to u/sildenafil_PRN on Reddit
Well worth a read,
@gmcuk
communications with government prior to HoL PA debate, including identifying any 'supportive peers'.



20
121
292
6
58
125
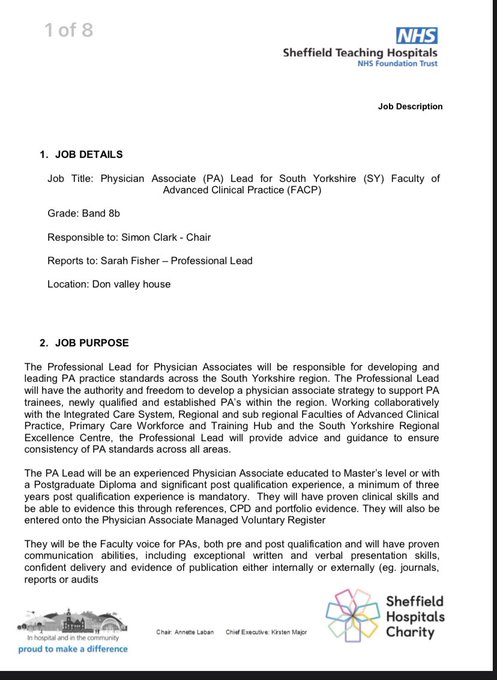
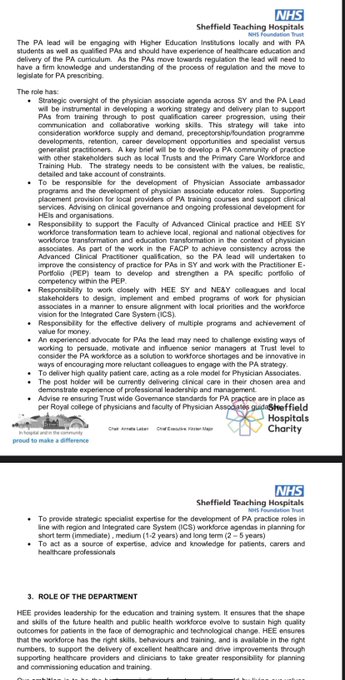
A job advert for what seems to be a propaganda/PR role for PAs. Band 8B!!
Could have hired a doctor or 2 for this much instead of trying to convince everyone to let underqualified people practice medicine

Band 8B PAs to :
‘Ensure that best practice is shared and adopted across the system making use of and contributing to HEE transformational tools. Challenge ways of working and persuade, motivate and influence other senior managers to realign their practice where necessary’
15
33
82
2
54
119
@nohandsup
It's topsy turvy.
PAs add nothing new to an MDT and can do less than a doctor.
Nurses are uniquely trained in the MDT. Nursing pay should start above PA pay. As should doctor pay.
The PA rollout, however, is an entirely political choice
2
15
122
@DocShivSharma
@Doctors_Vote
@KateAndrs
Absolute gutter journalism.
Acting as though publicly sent messages to all doctor whatsapp groups are a "scoop".
Oh, and cheltenham a&e closes evenings and bank holidays in normal circumstances. Selectively offering info, I see
6
6
111
This is insane.
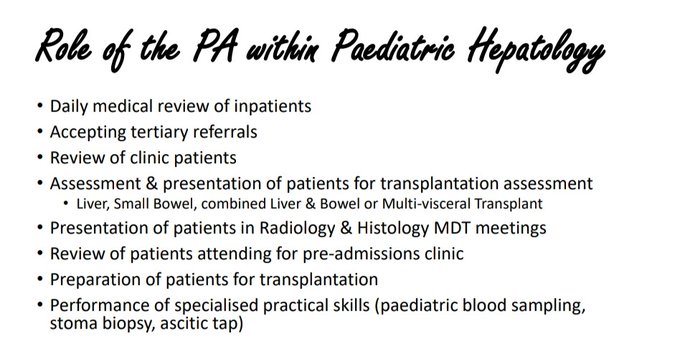
That big bbc article showing that PAs were staffing quaternary paediatric liver service rotas and giving advice?
It's been happening since 2019. And FPA-RCP knew about it.
Here it is from a presentation boasting about it at their 2019 conference 🤯🤯🤯
3
22
117
Twitter community notes went hard this time, and I'm here for it
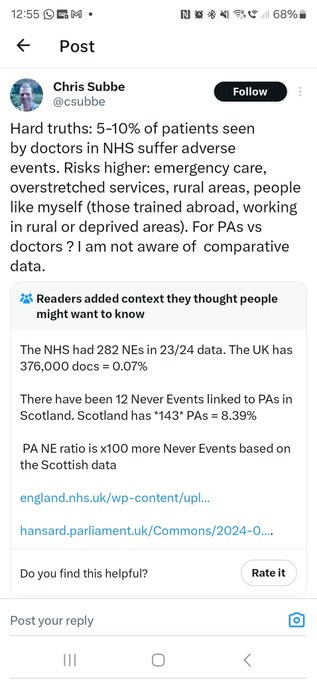

Hard truths: 5-10% of patients seen by doctors in NHS suffer adverse events. Risks higher: emergency care, overstretched services, rural areas, people like myself (those trained abroad, working in rural or deprived areas). For PAs vs doctors ? I am not aware of comparative data.
95
15
61
2
38
115
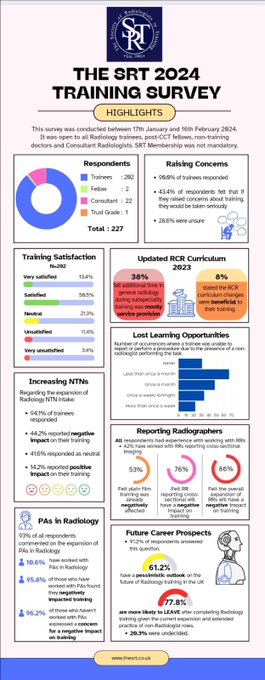
Number of take-homes here in an i sightful SRT survey. The
@RCRadiologists
would benefit from asking some of these difficult questions.
1. Any loss of training opportunity to a non radiologist is not acceptable when the buck stops with us.
1/n

Thank you to everybody who participated in the SRT UK Radiology Training survey!
Here are some highlights of the results, with a full report to follow soon.
#RadiologyTraining
10
71
147
3
33
110
Save this one for posterity.
Nursing leader denigrating and questioning the credentials of a CNS (specialist nurse) who doesn't happen to subscribe to the same ideas about specialist knowledge


2
1
19
4
9
107
Oh my, did anyone foresee this?

9
14
102
This is wild AF
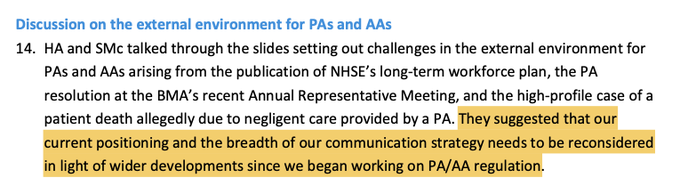
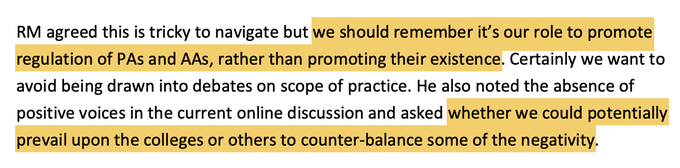
GMC knows about developments, and knows there is doctor opposition (pretending they think it's a vocal minority).
It also knows very few supportive doctor voices, so trying to promote/support those and outsource advocacy to royal colleges.
No integrity. See GMP

3. Indeed, they were specifically briefed on That Story during the summer, but have opted to keep an arm's length from the issue: "try recruit the Colleges to do a bit of Good Vibe PR instead". I wonder what the victim's family would say?
4
27
108
4
29
99
@gmcuk
As a doctor, I don't want you regulating them. RCR, BSIR and AoMRC have made similar sentiments known. You're ignoring us.
Also, you've said you're registering them, not regulating them or defining scope/competencies.
So you're contributing nothing to patient safety
1
16
103
@Dr_Done_
Very easily testable hypothesis - they do 5 years med school in 2 years? Get them to sit a med school finals exam.
4
3
102
@ClareGerada
@Jillyphys
@ExplosiveEnema2
@rcgp
I despair again at such a point. In no universe is a PA qualified to hold a doctor's bleep, unless to list numbers to the doctor can call back later.
If you can't see how inappropriate this is, you're contradicting the NHSE/RCP joint guidance saying PAs shouldn't be on a Dr rota
1
8
102
@InfoPars
Hi, non anon here. You might see this as a win.
But GMC granting faux legitimacy is a disaster.
Funny how this is viewed as a win for your egos, but utterly no regard for patients who are being misled into thinking that PAs have more knowledge & expertise than they actually do
3
12
100
Hi all, I've deleted my quote tweet about the tragic case at the royal berkshire on the advice of a doctor i highly respect.
I don't think I wrote anything I don't believe, but I'll elaborate further and offer some advice
1/n
5
12
98
Remember when the GMC caved into a racist media frenzy to strike off a Dr, so there would be "confidence in the profession".
Now they're breaching the very reason they were established; to ensure confidence that people seeing Drs are seeing someone qualified
#bearlyaregulator
1
28
99
This just confirms that even some PAs recognise they're scabs. Pushing thatcherist ideas about a free job market made in whitehall to weaken workers with too much power/vital skills.
Shame is, these gov lackeys don't actually have the qualifications/skills. Patients suffer

Interesting that the founder of
@UMAPsUK
sees PAs as "competition" with doctors
What happened to not replacing?

44
78
311
3
30
95
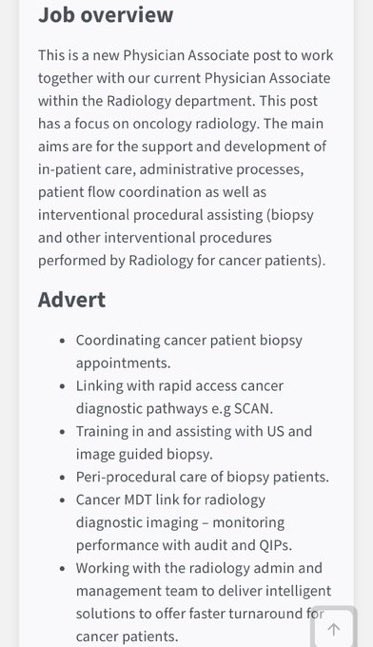
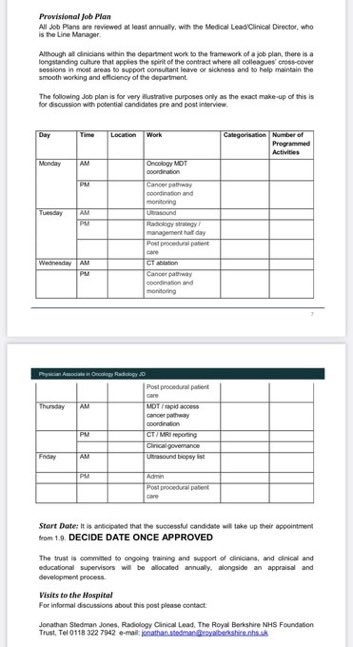
We undergo competitive application processes, rigorous sign-offs & famously robust exams to be deemed safe to any of this. (Even then, most are not expected to be level 4 for CT ablation at CCT)
Can you see why we're upset?
@halliday_kath
@DrStephenHarden
@Dr_PriyaSuresh
#PhysicianAssociate
#Oncology
#Radiology
Why & How Safe ?
@halliday_kath
@RBNHSFT
@lungdiagnosis
@JeanetteRCR
@TheBMA
@BSGAR_UK
@BSIR_News
@_the_SRT
@BSSR_Site
@myESR
14
48
135
9
15
95
This is one of the most horrifying things I've seen come out of recent MAP discussions.
This, in a field with stiff competition
28
26
120
6
29
97
@UMAPsUK
Undergrad doesn't count as it's not honed to be relevant to medical practice.
The CPD is exceeded by GP trainees in a matter weeks.
The post cert qualifications aren't defined benchmarks like postgraduate medical training. Vague/nebulous words to give impression of expertise
1
5
94
Why is this same little troll agency still being invited to recruit at events?
Hardly becoming of official communications

PA’s, pharmacists, paramedics and now nurses.
At this rate the dr-anon little crabs will start to come after the GP receptionists.
33
5
19
4
10
95
I love this. Illustrates quite well why some people's job in healthcare should remain within its remit.
In this case, even copy-paste or looking for a word to trigger a cost code seems a bit too cerebral

11
11
91
@ExplosiveEnema
@jeannie_watkins
@FPARCP
If this were a doctor (or any academic in a rigorous field), failing to declare a huge interest, not only would they have all their research called into question - there would also be disciplinary consequences.
2
7
85
Solidarity from, and with, the fire brigades union.
Deskilling by coopting a group of workers was known as scabbing, and unions recognise this when they see it.
Except, unlike keeping coal flowing (but less effectively), this group practices medicine & risks patient safety

At
@fbunational
Conference last week, delegates voted in favour of a motion by
@fbu_lancsfbu
seconded by
@fbumerseyside
to oppose the growing use of Physician Associates.
Deregulation and deskilling of all public sector organisations is something we must all fight together. /1

17
249
517
0
35
88
@Dr_Done_
Taking advice for some of the most dangerous patients to mess up with. I'm not intervening based on their advice.
No one should accept this as valid. I wouldn't want it for my family
3
11
88
@IncogAssociate
@RCPhysicians
@rcgp
Look at the sort of people who are your "allies". Try to reflect, please.
Are the IEA libertarian extremists & a hereditary lord of dubious morality/honesty really doing this in the interests of patients?
Or are you unwittingly being used as pawns in a bigger political game?
0
10
82
@SecretPhysician
@jabberwock951
@DrEilidhMaria
I'm more concerned they kept suggesting primary care/community management and no one clocked this patient ought to be sent to hospital until the GP saved the day.
Dearth of understanding of risk
2
5
85
@ClareGerada
@aashfaque14
@Cleverclog67596
@ExplosiveEnema2
@rcgp
That experience counts for nithing when working seeing undifferentiated patients.
An F2s admittedly minimal experience is still superior to any prior experience a PA had when it comes to seeing undifferentiated patients.
I despair at the dishonesty of your assertion
1
5
85
@beckstweetering
@GMB
@susannareid100
@edballs
False argument - if Drs who are better trained make mistakes, how can you suggest rolling out PAs with less training?
PAs are not NEEDED in any sense. There are enough doctors - the government just won't fund jobs for doctors but will for PAs
2
4
86
I think you'll find the BMA is the most democratic and representative body for doctors in the UK
The only organisation that can claim more members is the GMC - because we're forced to pay them to practice. You'll also find that we don't like how they're unelected & unaccountable


0
18
83
A thread to all clinicians looking at imaging and deciding on patient management secondary to it.
The theme:
Trust your clinical instincts!
Below is a nice os subfibulare. Imaging request said patient had pain over the MEDIAL malleolus. But sent home from ED in a walking boot

3
9
82
No additional strike rounds have been called.
@VictoriaAtkins
@DHSCgovuk
can you please do your jobs and get on with this? Surely this should be a priority for the SoS for health?
What on earth else do you have scheduled that takes precedence?

@TTOTrainee
@VictoriaAtkins
@TheBMA
@RobLaurensonD4P
Negotiations have not restarted despite the seemingly abundantly clear position the Government were ready.
We are waiting and ready to restart as soon as they are.
We will keep doctors updated with developments.
24
185
586
5
17
80
This. Just this.
Message to GMC, NHSE, FPA, RCs - you had your chance to prove you cared about medical standards & patient safety.
Cry more


0
10
78
Many thanks to
@drmattuk
for bringing this tragic case to light.
Keep up the fight.
For patients
And for the profession
6/6 end
1
5
79
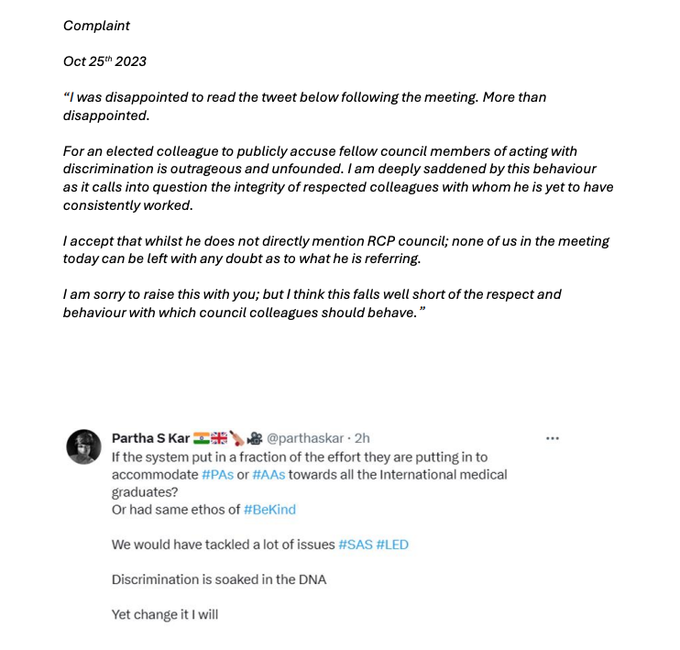
I wish I knew the RCP councillor who complained about Prof Kar's tweet below.
Not for a trial by media. But physicians deserves to know who they may be voting onto council. Who has these views hidden behind the safety of a screen/anonymous complaint?
Respect to prof Kar 🙌🏼

Now that it has been 'looked into' & thrown out?
Let me share with all a formal complaint
From within Council
@RCPhysicians
Tactics people use to shut down raising issues around IMGs
Kids-please note!
Beyond my parents? I don't give a fig about anyone else's 'disappointment'
57
88
514
2
13
75
Until then, keep raising concerns, and don't be cowed.
The gov's workforce plan is a dangerous experiment with the lives of the british public who can't afford private healthcare. Replacing Drs with the less qualified a betrayal of patient trust & patients DO deserve better
4/5
2
13
77
@drmattuk
@fascinatorfun
@GrumpyOldDoc
@GMCharlatan
@medicalmodelbri
Honestly, despicable. Surely this should be perverting the course of justice/malicious misuse of police time?
Like the other comments, I'm in for any crowdfunding
0
6
76
A propaganda push to belittle the views of doctors as expressed in every single sampling there has been so far.
Bravo on the piece which, if true, would make your department an exception used to rubbish concerns of Drs nationwide.
Reprehensible stuff

1/4 It is sad to see the very public onslaught on Physician Associates. We are a unit with a proud history of teaching, training and investing in our junior doctors at all levels. We are an
@RCSnews
accredited fellowship training centre in Robotic surgery (
@IntuitiveSurg
)
2
35
159
1
13
73
@SecretPhysician
Yep if you're dependent on doctors to work, they must call the shots about your scope of practice.
A trainee's scope is also determined by the responsible consultant.
The problem with expanded scope thus far has been irresponsible consultants (and trusts and DHSC)
0
6
78
Unbelievably despicable behaviour.
Maybe the
@gmcuk
should reflect on how its processes are so harmful for Drs that some are weaponising referrals
3
13
74
This is an important and oft neglected point.
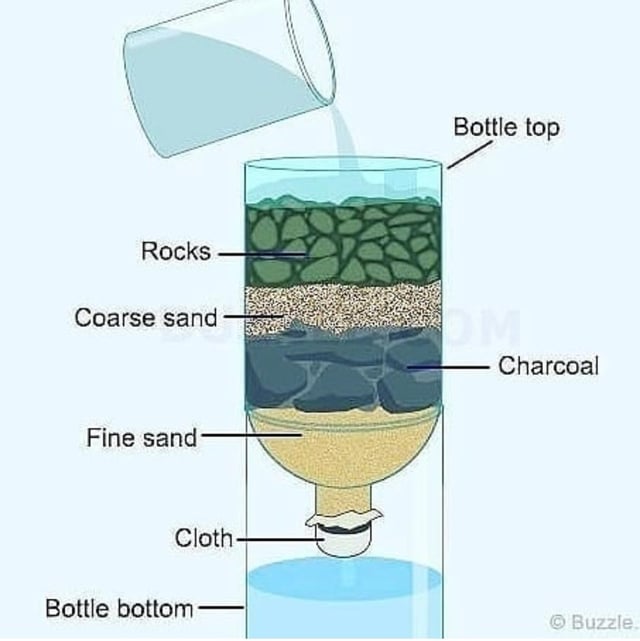
Our exams can be hard, especially the post grad ones. But passing (admittedly rigorous) exams without doing the rest of medical training doesn't make you a doctor or equivalent

@JonnyGucks
Neither
Exams are just one of many filters. That's why opening up exams to non-medics is a terrible idea. There are a litany of other barriers Drs have to pass to get where they need to be
Would you drink water filtered just through the rock layer?
8
16
78
2
6
70
These guys need to understand what rebuttal means. There was an internal investigation at the hospital.
@JanetEastham
if this organisation is questioning your journalistic integrity, could the paper please, perhaps, take them to court for libel?

REBUTTAL
The Telegraph Article from 27/01/2024: "Physician associates accused of illegally prescribing drugs and missing diagnoses."
#physicianassociate
#anesthesiaassociate
#maps
#umaps
#medicalassociate
0
16
16
1
17
71
@glurcher
@scrivvyfloor
@dr_lungs
@sh_abbers
@dannyjnwong
@pcricoarytenoid
The issue is the taskification of medicine into little aliquots of doctoring, protocols/pathways & tasks that can be done by technicians without the same education & training.
It's not medicine. They're not clinicians. It's a supervised technician.
3
15
71
@RCPhysicians
@NHSEngland
It is implied that a PA shouldn't be on a doctor's rota. I applaud that, but it's not enough.
I would much rather this was made explicitly clear. Lest some hospitals interpret it liberally (which we all know they will try)
5
15
70
@karimbrohi
I suggest you reflect on your rather rash defence of your trust's suggestion, and the subsequent valid critiques of it.
Medical students need advocates. Ones who will remind the trust that this proposal requires costing. This isn't 7/7, this is a failure of a contracted operator
1
6
70
@vcg239
@LittlePersonDoc
@timricketts_
@alisonleary1
@CheGuevera27
@ShaunLintern
This is mad.
Forget a chip on her shoulder, this is a tonne of potatoes on her back.
The denigrating & bullying language from someone who will then champion "bekind".
Classic NHS leadership. No wonder we're in this mess when she turns on you instead of respectfully engaging
1
3
68
@EileenBurns13
Prof Greenhalgh has been nothing but professional in this whole discussion and as far as I can see, those expressing an interest in co-signing to raise concerns have done so with utmost courtesy.
Why the caveat?
4
3
66
@IncogAssociate
You're not ordering anything. It's not personal - nobody does technically.
And I certainly hope nobody is accepting requests from you for imaging without the patients being seen by someone better qualified
3
7
67
@anonPA5
@dx_mighty
Why is there a risk of being reported to the med school? And what's the relevance of bringing up that she's a mother?
No one even suggested this, which makes it look like a threat.
"Lovely kids and career you have there; would be a shame if something were to happen to them"
1
0
69
A very important thread.
What she's describing is appalling, but the themes are seen time and again across the NHS.
I mean this in terms of management attitudes towards doctors, patient safety, and adequately qualified staff

I'm leaving my current role in a community hospital due to safety concerns that have not been addressed adequately. I'm sharing this because I'm deeply concerned about what is happening in the NHS and I'm worried about the risk our patients are facing.
120
2K
6K
2
6
65
If there were outliers, that should be ironed out over the course of a larger sample size.
N numbers are the antidote to exceptions, after all.
But even then, hosp management refused to approve this. They don't want someone to scrutinise this data.
Tip of the iceberg
2/2
4
11
66
@Plyons251
Parking charge notice is not a penalty charge notice.
It's a lot more legal hassle for them to demand payment.
NHS hospitals basically source their parking enforcement to private companies. They rely on spooking people into paying without challenge. But know your rights
2
3
66
@Dennisw99863685
@MichelePaduano
You can be a technician. The technical skill isn't hard.
A flamenco guitarist probably has better manual dexterity than most doctors, PAs or ACPs. But you wouldn't teach them to do a chest drain or lap chole without a medical degree
2
2
63
Over 700 shifts.
Equivalent to 2 and a half doctors' annual shifts.
Yet Dr jobs are limited while there are willing candidates.
All while claiming they "struggle to recruit" to justify having underqualified folk filling doctor shifts

1
16
65
@Xeon4f145d96s1
@gmcuk
If their own staff are confused, what hope do patients have?
Except the whole point of the role, its renaming, and the pursuit of gmc registration was to create this kind of confusion.
It's sinister
2
6
63
@Dr_Done_
It's a lie as well.
If we're being pedantic (i.e. understanding that language matters), a clinician is, by definition, a doctor.
Another attempt to trick the public into seeing underqualified folk.
We can all see that's the aim of this charade
1/2
2
8
64
@iDrSunny
And if we're talking about them doing the same job, who does that role more effectively and with more expertise?
It's such a false economy
2
6
63
Anyone wondering why some docs go anon - there are some pretty vindictive people out there. People who disagree or don't like your tone and choose to make your life harder with a vexatious GMC referral.
They get REALLY frustrated when they can't use that threat. See below

LOL please guys. I'm shaking.
If my identity comes out I'll go with it. Bank details? Ive been a doctor in the UK, there's not much in there.

62
27
468
0
7
61
@Xeon4f145d96s1
BSG will need a colonoscope to search for whatever morsels of dignity might be left after this
4
6
63
@BMA_James_Steen
@MandloiJaideep
The issue is if you have a weak or complicit clinical supervisor, they will flag it as "poor teamwork" or "interpersonal relationships" and make obstacles for your progression.
DiTs need to be strong, but you need consultant support or some imposition of standards from higher up
3
1
58
@glurcher
@scrivvyfloor
@dr_lungs
@sh_abbers
@dannyjnwong
@pcricoarytenoid
Yes. Yes they are. I think that's what attracted so many comments on your original post.
Because of healthcare policy to undermine Drs & break our monopoly. And lazy consultants who would rather train a technician just once to relieve them of a task/training the next generation
3
5
62
@quackophage
I'm in awe
@quackophage
, amazing work getting this FOI and getting it out there.
One positive of all this is that it shows they ARE scared of doctor opposition, and they recognise that their plans have significant obstacles if we don't comply.
We all know what we need to do
0
9
59
Interesting that
@CQCProf
have now been coopted into the ruling regime's diktat.
Do
@prof_standards
have anything to say about this? Or are they toeing the line as well? CQC aren't doing their job
The courts now seem to be the only recorse. Wishing you success
@AnaesUnited
!
‘PAs are generalist healthcare professionals who are trained to the medical model ‘
When the
@CQCpressoffice
release an update on physician associates in General practice with propaganda straight from
@FPARCP
@NHSE_WTE
then what hope do we have ?
@doctor_oxford
@parthaskar




28
94
256
2
32
59
If they were honest about capabilities, patients might be routed to nearby alternative MTCs.
But no, because that would lose some income stream and embarass some managers.
So other managers anonymously leaked info.
If you're not scared you should be
2/2
1
6
51
@Ask_foradoctor
I tell PAs they can call the secretaries, or get a doctor to call me.
Inappropriate, when radiologist time is limited, and with the risk of ionising radiation, for the risks/banafits to be discussed with someone who doesn't grasp either
2
4
58
@DrAsifQasim
The greatest cost demanded by this career is not, in fact, any of the above.
It's our youth
5
6
59
Important perspective in this whole debate.
Medical educators have let down PAs & missold what the course actually prepares them for. Not everyone will have the insight to realise this as early as the OP.
PAs have a right to be angry/upset.
3
25
59
So I'm commenting because if there is a cover up as was suggested, I really REALLY want examples to be made of people. If that's the case, the repercussions have to be prohibitive enough that trusts become more likely to come clean than hide wrongdoing
3/n
2
3
56
@ExplosiveEnema
@Ormerod84
@LocumPA_Ltd
@RCPhysicians
@FPARCP
Some of the comments are missing the point.
The big issue here is that this company:
1) Advocates for unsafe scope for PAs
2) Sponsors RCP giving a RCP a clear COI regarding the topic of PAs and scope - because of point 1
0
7
55
This is now 3 resignations that we know of thus far.
It seems the RCPL is losing those with integrity.
Those in the leadership who remain have a short window of opportunity left to resign with dignity
#RCPEGM

@jfnephlolz
@FutureHealthJ
@RCPhysicians
I wasn’t planning to publicise it but, in light of your announcement, I can say that I resigned from the Advisory Board of Clinical Medicine last week, for the same reason.
12
192
837
2
14
53
@ellorakamineni
@JoshuaSoane
To be terrified you have to understand how many gaps there are in your knowledge and understand the gravity of missing something crucial.
In their cases, they learn a few patterns of presentation, a few guidelines and protocols, and crack on. The bliss of ignorance
3
1
53
@Dababydoc
@r1chardf1tzg3r1
Mad thing is she was RCP president during last JD disputes/IA when they sent out shameful communications blaming JDs for the strikes.
In 2015, she set up the Faculty of PAs. Workforce plan seeds planted then.
Anti-doctor to the core
1
6
52
Spotted this on reddit, and thought of my favourite meme writers on twitter to be up to the task
@mouseter_chef
@ExplosiveEnema2
@GMCharlatan
5
4
53
@FrankCoffey26
I was going to say, this does not constitute bullying in any form. No individual has been targeted. It's a joke about safe practice.
But, this account summarised it with much more panache

Roses are red,
The jokes not that serious,
To think this is bullying,
Is rather delirious.
1
3
28
1
4
53
Care to comment why the majority of your trainees felt workload & training were inadequate in the most recent training survey?
While you're at it, could you also make the soulless corporate messaging less blindingly obvious?
There's a saying somewhere about glass houses

@GeorgesUrology
@RCSnews
@IntuitiveSurg
Our Physician Associates are outstanding and an absolute asset to the dept . They are fully engaged ,caring,are permanent members of the team , well trained,learn skills quickly . The NHS would do well to embrace them as essential contributors to patient care .
0
10
66
4
8
53
@UKGastroDr
@Molly2323232323
PA locum ahency PATH allows PAs to accrue points for hours worked that they can then use to... wait for it...
Get private health insurance!
So that even PAs aren't treated by their colleagues. You couldn't make it up.
@iDrSunny
2
5
52
@iDrSunny
@PAsRTSolution1
@pppforpatients
You cluld train anyone to do the technical skills. Get a pro gamer and their fingers would smash through our lists.
But we don't treat real patients like video games. That's why we don't want standards watered down.
15/end
3
7
53