

Othman Al-Sawaf
@Othman_Al_Sawaf
Followers
1,214
Following
571
Media
65
Statuses
185
Emmy Noether Group Leader @CECAD_ Physician-scientist, Haematology & Medical Oncology. @UniCologne Visiting Scientist @TheCrick @SwantonLab
Cologne
Joined December 2018
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
#FNS歌謡祭夏
• 599199 Tweets
Chan
• 222697 Tweets
Bozkurt
• 206264 Tweets
#SnowMan
• 142042 Tweets
wonwoo
• 131783 Tweets
#WeAreSeriesEP14
• 125112 Tweets
Lagos
• 100917 Tweets
PondPhuwin WeAre EP14
• 81691 Tweets
#BREAKOUT初披露
• 68981 Tweets
POISON
• 38607 Tweets
フジファブリック
• 37787 Tweets
うたプリ
• 32872 Tweets
スタトレ
• 31585 Tweets
紫耀くん
• 28125 Tweets
ムーンシャイン
• 25236 Tweets
最高のパフォーマンス
• 22519 Tweets
リングライト
• 18987 Tweets
I'm a Dreamer
• 18681 Tweets
推しの子
• 17760 Tweets
ラウちゃん
• 14961 Tweets
チアリーマンズ
• 14736 Tweets
HYDEさん
• 14672 Tweets
相葉くん
• 13299 Tweets
心霊番組
• 11346 Tweets


















Pinned Tweet

So glad to see this out today in
@NatureMedicine
- it was an amazing journey!
Endlessly grateful to the team
@Swantonlab
and especially to
@MariamJHanjani
and
@CharlesSwanton
for their guidance & mentorship.
Check out the tweetorial below! 👇

Cachexia is a devastating condition in patients with cancer. Our study on cancer cachexia in
#TRACERx
is out today in
@NatureMedicine
led by
@Othman_Al_Sawaf
,
@MariamJHanjani
,
@SwantonLab
:
Key results in a brief 🧵
1
94
255
10
10
63
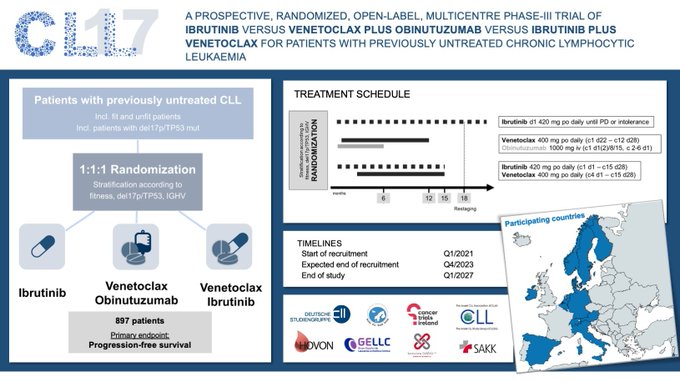
It's a wrap! Delighted to announce the final patient was enrolled in
#CLL17
! 14 months ahead of schedule.
909 pts randomized to cont ibrutinib, FD ibrutinib-venetoclax or FD venetoclax-obinutuzumab.
Thank you to all pts, study teams & collaborators for this huge milestone!

22
23
173
Excited to announce I received an Emmy Noether fellowship from
@dfg_public
to set up a research lab 🔬 on the evolution&plasticity of
#CLL
& other
#cancers
@UKKoeln
@CECAD_
Cologne🇪🇺🇩🇪!
Fully funded PhD student & postdoc positions available-get in touch to connect via email&DM!

31
17
166
After 3 years of preparations, the first patient was enrolled on the CLL17 study today! Thanks to all patients, their families, nurses, physicians and investigators for joining us across 13 countries in this exciting journey!
@HallekMichael
@DrMDavids
@tobyeyre82
@LukasSmolej
11
20
116
Parallel to a fantastic
#CLL
session
#ASH23
, the primary analysis of the RT1 study just went online
@NatureMedicine
: High efficacy + tolerability of combined PD1+BTK inhibition with tislelizumab+zanubrutinib in patients with Richter-Transformation

11
22
94
Check out our latest work on transcriptomic profiles of
#CLL
, drivers of MRD response and 5-year results from CLL14 – all out today in one paper
@NatureComms
:
Key results in a brief 🧵
4
26
84
Delighted to share our latest paper in
#JCO
, in which we suggest an MRD growth model of CLL, including new data from the CLL14 study (Ven-Obi vs Clb-Obi).
#leusm
#GCLLSG
@ASCO_pubs
Some results in a quick 🧵 1/n
1
12
71
Wonderful few days in ☀️Houston, attending
#SOHO2023
and discussing MRD & CLL.
Also saw some rocket science - both at
@MDAndersonNews
with
@NitinJainMD
(thanks for showing me around!) and at the NASA museum!




1
3
55
Interesting study by
@NitinJainMD
et al
@CCR_AACR
, on absence of BTK,PLCg, BCL2 mut in post-Ven-Ibru relapses:
Has implications for re-treatment concepts!
Also check out commentary
@DrMDavids
and I wrote on this important topic:

2
15
52
The phase 2 CAPTIVATE study has longer follow-up plus a considerably bigger I+V cohort than GLOW.
👇 This is from 4-year Captivate data on I+V (Ghia et al ICML 2023). Clear correlation of EoT-MRD with PFS also for Ibrutinib+Venetoclax in my view….


🤔 Minimal Residual Disease not associated with progression-free survival outcomes after fixed-duration Ibrutinib-Venetoclax vs Chlorambucil-Obinutuzumab in the GLOW study in
#ChronicLymphocyticLeukemia
➡️
#CLL
#Leusm

1
6
13
1
11
49
One of the best
#CLL
conferences I’ve ever attended - thanks
@DrMDavids
and the
@DanaFarber
&
@iwCLL
teams for hosting us and for setting up such a great agenda! Flying home with many new ideas and collaborations in the works 🛫

Honored to contribute to the conversation, and I come away from this meeting with renewed energy and inspiration to continue to work toward cure for patients with CLL!

0
3
57
0
3
46
Had a wonderful visit to Buenos Aires last week to meet amazing haematologists and discuss CLL management, research and future strategies. Thanks so much for the warm hospitality and great discussions!
@silcugliari
@MiguelPavlovsk6
@Rocustidiano
@ValeAntico
@Bautischenone




6
4
46
Interesting study by Malcikova et al in
@BloodJournal
, demonstrating shorter OS of patients with CLL and low-burden TP53 mutations:
Also have a look at our commentary in the same issue: TP53 mutations in CLL: does frequency matter?

0
10
46
Highly recommend these two books by
@VPrasadMDMPH
/ Prasad and
@adamcifu
- some controversial topics, but excellent food for thought and very relevant to oncology & medicine in general.

0
7
43


Very exciting data, congrats to the UK CLL group!
Intriguingly low tox in the I+V arm (vs GLOW), despite I+V tx duration being ≥2 yrs in most pts. Age seems to matter here.
Do you have a plan on how you'd implement this outside of studies, given the fixed-dur I+V label🤔?

#ASH23
abstracts out! Here is a highlight:
Check out this from the FLAIR
@NCRI_partners
trial
MRD-directed Rx length of Ibr+Ven vs FCR phase III RCT
Massive PFS adv + OS benefit for Ibr-Ven
#CLL
#lymsm
Congrats to all UK investigators, Tal M and Pete H.

8
28
125
2
6
42
Check out this review article that I had the pleasure of writing together with John Seymour, Arnon Kater and Kirsten Fischer, now published in Hematology/Oncology Clinics:
👉 Should uMRD Be the Goal of Chronic Lymphocytic Leukemia Therapy?

2
11
40
Thank you
@cancertrials_ie
&teams for this great effort! Had a wonderful opportunity today to meet with Patrick Thornton,
@amjad_hayata
and many
#CLL17
investigators in Dublin 🇮🇪- a huge honour and privilege to have such committed partners in
#CLL
research!


Today is World CLL Day
#WCLLD22
The CLL17 trial, opening in 🇮🇪 just 16 months ago has recruited an incredible 81 patients, more than double our target (40). Enormous congrats & goodwill to the sites involved & patients on the trial!! 👊👏
Trial details:

0
12
37
1
5
37
Join us at the XIIth
#GCLLSGworkshop21
from April 29 - May 1, chaired by
@HallekMichael
!
3-day program on all things CLL & free registration at
Great faculty with
@DrTonyLetai
,
@DrMDavids
,
@wwierda
,
@NitinJainMD
,
@anthonymatomd
,
@jeff_sharman
& many more!

1
13
37

Nice study by
@herishanu
et al
@BloodJournal
on Covid-vax in CLL:
- response rate 40% in 167 pts
- response in tn > rrCLL; under treatment<remission
- response with BTKi and Bcl2i+CD20 impaired👇
=> CLL pts should receive vax whenever available
=> booster?

1
9
32

What a great start to the 2nd day of
#GCLLSGworkshop21
!
Inspiring discussion between John Seymour and
@HallekMichael
-fascinating insights into John's personal career path, advice on mentorship and above all how his determined work lead to the establishment of BCL2i for CLL.


0
3
33
That's it for this year's
#GCLLSGworkshop21
- thanks to all speakers and attendees for great presentations, input and discussions!
Talks on-demand at .
We'd love to hear your feedback - just drop a DM or email cll-studie
@uk
-koeln.de, we appreciate it!

3
5
31
Fantastic lecture by
@DrMDavids
on TP53 aberrations in heme malignancies at the
#ASH21
Presidential Symposium. Congrats Matt!
#leusm

0
1
30
It's going to be a very exciting
#ASH21
! Lot's of interesting data from FLAIR, ALLIANCE, SEQUOIA, CLL13, Captivate, Glow, and many other CLL studies:
#leusm
@tobyeyre82
's tweets are such helpful summaries👇
CLL13
Eichhorst et al
926 TN 1L fit pt
1:1:1:1
150 FCR ≤65y 79 BR >65y
237 VenR
229 VenG
231 Ven-I-G
fup 27.9m
Co-primary endpt 15m PB uMRD
⬆️ in Ven-G vs CIT: 86.5% vs 52.0%
⬆️ in Ven-Ibr-G 92.2% vs CIT
VenR cf CIT
Time-limited Ven-G or Ven-Ibr-G ⬆️ 15m uMRD vs CIT
#ASH2021



1
8
32
0
5
28
Look who I ran into today 🇩🇰- had fabulous meetings with
#CLL
maestros
@carsten_niemann
@caspardcb
@Rigshospitalet
in Copenhagen and
@TobiasREberlein
and the haem team @ Regionshospitalet Gødstrup to discuss all things CLL and future collaborations. Thanks for having me!




1
1
28
@VPrasadMDMPH
@AaronGoodman33
Allow me to summarize the systematic
#GCLLSG
approach for 1L CLL tx, which reflects this spirit:
1. CLL5 showed Clb = Fluda
2. CLL11 showed ClbO>ClbR>Clb.
3. CLL14 showed VenO>ClbO,
4. CLL13 showed VenO>VenR/FCR/BR.
5. CLL17 is randomizing VenO vs VenIbru vs Ibru
4
3
27
Further Covid-vax-in-CLL pre-print:
@low_helen
et al from
@unibirmingham
report antibody response in 299 CLL pts:
- after 1st jab only 34%, after 2nd 75%⬆️
- w&w: 83%
- on BTKi or prev CD20ab: 21%
MV analysis: BTKi + low IgA assoc with ⬇️ ab

1
5
27
Now online ahead of print in the Am J of Hematol, our analysis of quality of life with/after Ven-Obi vs Clb-Obi in 1L CLL - main conclusion: No impairment of QoL and slightly earlier symptom relief with Ven-Obi.
#GCLLSG
0
7
24
New paper from
#Hovon
CLL group
@TheLancetHaem
- 12x Ven-consolidation after 12x fixed-duration Ven-Obi:
- Rando: 12x Ven-Cons regardless of EoT-MRD status vs MRD-guided 12x Ven-Cons
- No diff in MRD-status after Cons (!): In both arms, uMRD rate was ~50%


3
6
24
Wonderful news! Thank you all for the great enthusiasm and support - all
@cancertrials_ie
sites are recruiting exceptionally well and the collaboration has been a delight from the very beginning.
#GCLLSG
#CLL17
#leusm

First patient enrolled on
#CLL17
thanks to the hard working CCTU team at UHL
@ULHospitals
@ulresearch
And team
@cancertrials_ie
with GCLLSG
5 more patients in screening 🙌 chemo free CLL frontline
@CllIreland
@BloodCancerIRL
@Othman_Al_Sawaf
3
4
76
2
6
23
شكرًا جزيلاً لك
@Kuwaiti_Dr
على الدعوة والمشاركة في المؤتمر ومركز الكويت لمكافحة السرطان الممتاز.أتمنى لكم كل التوفيق و أسأل الله أن يوفقنا وإياكم لكل ما يحبه ويرضاه.
It was my pleasure to visit the impressive Kuwait Cancer Control Center. Looking forward to future collab!

ما بعد المؤتمر
تشرفنا بزيارة د عثمان الصواف
@Othman_Al_Sawaf
من جامعة كولون - ألمانيا للمركز و مناقشة الحالات في اجتماعنا الاسبوعي multidisciplinary team meeting

0
2
2
2
1
21
Had a great chance to catch up with the Swedish
#CLL
group
@karolinskainst
in Stockholm today - thanks Mattias Mattsson, and
@rosenquistbrand
for hosting me, looking forward to further collaborations! (Very stylish campus!)




1
1
22
First time attending the
#CrickCancerConf
@TheCrick
(and first in-person conference in ages…) - fantastic program and great speakers!

0
0
22
Glow-study
#EHA2021
late breaker: TN elderly/unfit CLL pts:
- 106 pts 3x I+ 12x IV: mPFS nr
- 106 pts 6x ClbObi: 21 m
- PB uMRD: 55% vs 39%
Looking forward to Arnon's pres - def a lot to consider, uMRD somewhat lower than IV in Captivate (77%, Abs S147)

1
4
22
Elevate-RR: Acala vs Ibru, similiar efficacy, less cardiotox with Acala (fewer AF, hypertension, bleeding), although this seems to be relative risk reduction (bleeding rate 38% vs 51.3%, so still something to be cautious of when using any covalent BTKi)

0
1
22
Great meeting with Arnon Kater, Marjolein van der Klift and Evert-Jan de Kruijf
@OncologieTV
- always a pleasure discussing CLL, MRD and clinical management with our colleagues from the Netherlands.
Looking forward to
#GCLLSG
&
#HOVON
collab in
#CLL17
!

0
2
21
The XIIth
#GCLLSGworkshop21
starts in 45 minutes!
You can still register for free at !
Check out today's exciting agenda 👇

1
6
21
Fabulous news! Thank you for the intense preparations over the last couple of weeks - this is a great milestone for the whole CLL17 project. Looking forward to many enrollments from Ireland!
@CllIreland
Congrats
@UHW_Waterford
who today became the first Irish site activated on the CLL17 study! Well done to everyone involved 👏👊💪
Once fully open the trial will offer a new treatment option to 40 eligible 🇮🇪 patients with previously untreated chronic Lynphocytic Leukemia (CLL)

0
10
43
1
2
19
Very much enjoyed the breakfast meeting with
@DrMDavids
at
#SOHO2021
- great discussion on MRD in CLL! Thank you to
@SocietyofHemOnc
& the attendees, see you at
#IWCLL2021
next week!

0
2
19
Last day of the
@CancerGrand
#CANCAN
retreat in
@CSHL
- three days of amazing science and new collaborations. Thank you
@EileenWhitePhD
@MarcusDGon
@JanowitzTobias
for hosting us and bringing us together!


0
2
19
Great performance indeed! Thank you to the patients & sites and of course
@cancertrials_ie
for this great effort!
Looking forward to the next months & years of close international collaboration!
#CLL17
#GCLLSG
Mighty congrats to everyone involved in CLL17 (for patients with previously untreated Chronic Lymphocytic Leukaemia) Info here:
Since mid-April 14 patients accrued @ 5 active sites (& 3 more sites due) & 8 patients in screening.
What a performance!👊👏

1
4
23
0
2
18
Have a look at our Trial-in-progress
#ASH21
poster
#2634
, presented by
@DrMDavids
. The phase-2 ReVenG study explores Ven-Obi-re-tx as 2L in CLL. Great collaboration between
#GCLLSG
#DFCI
and AbbVie+Roche/Genentech. Details:


0
4
17
Interesting paper by
@hjcherng
&
@NitinJainMD
- Outcomes of CLL AYA pts. Median 37 yrs, 10-yr-OS ~77%:
First tx lines can be quite straightforward in my exp, but when pts reach 50, salvage options become rarer. Still a lot of work to do for CLL community.👇

2
3
16
New paper on outcomes of pts with CLL+TP53 aberrations after limited duration tx by
@PaulaCramer20
#GCLLSG
in Blood - based on pooled phase 2 cohort, after treatment cessation median PFS was >2yrs with high uMRD (>80%, esp after Ven-Obi).
Congrats Paula!

0
0
15
📢 New job opening in the lab!
We are looking for a PhD student with a computational background and interest in AI-driven data analysis 🔬💻🧠:
DM/📨 to get in touch!

0
10
15
Wonderful discussion after the first session of the XIIth
#GCLLSGworkshop21
- thanks to Cathy Wu,
@DrMDavids
@DrTonyLetai
, Arnon Kater and Ignacio Martín-Subero for sharing and discussing their insights!
Next session starts in 30 minutes at 6.15 pm CEST - see you there!

0
2
14
Amazing study by
@AbdelWahablab
@TaylorJ_MD
and colleagues - First description of resistance mutations in BTK that impair the binding of non-covalent (interestingly also covalent!) BTKi. Very cool paper, congrats also
@anthonymatomd
and team!


Overjoyed to share our lab’s new publication in
@NEJM
, a collaborative effort w/
@abdelwahablab
, led by
@ewang2323
, Xiaoli Mi,
@MCThompsonMD
& major contribution from
@SkyeMontoya
Mechanisms of Resistance to Noncovalent Bruton’s Tyrosine Kinase Inhibitors
34
41
266
1
0
14
Looking forward to participating in this sesseion together with Talha Munir and Jennifer Brown on April 25th!
Check out the agenda of this fantastic meeting at

The BSH 2021 Virtual ASM 25 – 28 April 2021 covers all the haematology specialities. Sessions will be recorded and available to view for a year. Discounts for BSH members. Register now.

0
1
6
0
2
14
Great symposia by Petra Langerbeins, Paolo Ghia, Kirsten Fischer and Eugen Tausch!
Interesting perspectives on BTKi, BCL2i, continuous and fixed-duration treatment.
More on that and many other topics tomorrow - don't miss it!


0
1
12
And of course:
#001
: Henry Kaplan Memorial Lecture by
@HallekMichael
and
#002
: John Ultmann memorial Lecture by
@AshAlizadeh
, a great
#GCLLSG
supporter & collaborator.
Promises to be an exciting meeting!
0
0
12
Interesting results by Rogers et al - in case of ibrutinib intolerance, drug class switch not always warranted. Switch to other BTKi seems to be sensible in some settings (Ibru -> Acala):

1
1
12
Thank you
@laird_barry
for hosting us in 🏴 & for the amazing
@CancerCachexia
conference - so many exciting data and discussions already!

And they say oncologists don’t get Cachexia - an exemplar advocate that they do by Othman Al-Sawaf
@ucl
@MariamJHanjani
@CharlesSwanton
#tracerX
@CancerCachexia
#ccs23

0
3
22
0
2
11
👉CLL pts should receive vax whenever possible.
Delay of CLL treatment after vax might be sensible in individual cases, however, this report shows that pts with planned treatment (i.e. active disease!) have impaired ab response=>well-controlled CLL is critical for vax success.
1
1
9
Very useful guidance by
@ADesaiMD
,
@VivekSubbiah
and co-authors on Covid-19 vaccination in cancer clinical trials: in
@NatRevClinOncol
For CLL trials - vaccinate whenever vaccine is available 👇
#leusm

0
2
10
Congrats
@anthonymatomd
+ coauthors on this important work-Pirtobrutinib in rrCLL 63% ORR, also post-Ven. I like the incl of pts with cardiovasc events on prior BTKi, AF, anticoagulants-tox profile remained very favorable. Looking forward to phase 3 data!
0
0
9
Fully agree, in
#CLL17
we encourage use of Covid antibodies and also Paxlovid when indicated (with necessary dose adjustments for Ven and/or Ibru).
0
3
9
@nico30f
@tobyeyre82
@GuiperiniMD
@cytohance
@Anthonymat
We usually do 1g acetaminophen po and H1 blocker, e.g. diphenhydramine 50 mg, 30-60 minutes before start of obi infusion, and 100 mg prednisolone iv or equivalent before obi. Start with slow infusion rate and consider giving 100 mg obi on first day and 900 mg on second day.
0
0
9
Last session for today starts in ten minutes!
"How I manage..." with a great line up of speakers focussing on all aspects of clinical CLL management.👇
#GCLLSGworkshop21

0
0
9
@lymphomahub
Not sure this is the ‘biggest’ difference. They are phase III vs II, they have different randomisations, primary endpoints, patient populations, sample size,…In
#CLL14
we are trying to answer other questions than in Captivate, so caution when comparing these two datasets.
1
0
8
Day 2 of the XIIth
#GCLLSGworkshop21
starts in 45 minutes with a fireside chat between
@HallekMichael
and John Seymour - live stream at !
#leusm

1
3
8
Final day of the
#GCLLSGworkshop21
starts in 30 minutes - live at . See you there!
Today's agenda 👇

0
1
8
@jeff_sharman
Fully agree, I think this is the first randomized dataset on I+V in young/fit patients, so pretty encouraging
0
0
8
Cardiovascular or immune-related AEs were very rare, most toxicity was related to grade 1-3 haem tox or grade 1-2 GI disorders.

1
1
7
@outschoolwriter
@CllIreland
@gmcrotty
@RuthClifford5
@EibhlinMulroe
@orlabdolan
@cancertrials_ie
@BreakthroCancer
@Paulkellyie
@DrHealeyBird
@DrRobertOConnor
Yes, sessions are available on-demand at shortly after the live-stream!
#GCLLSG
#GCLLSGworkshop21
2
0
7
@tobyeyre82
Agree, I am also a bit puzzled by the data, looking forward to Pete's talk.
Elevate-RR (45% TP53mut/Alpine ~12%) reports median PFS of 38m (Alpine <24 months) 🤔. ORR is not an ideal endpoint for a phase 3 CLL study.
1
1
7
Helpful report on IRR with Obi by Bourrier et al
@v_banerji
👇
IRR ⬇️(6%) when splitting 1st dose over 2 d (100/900 mg) + starting with low rates (6mg/hr, up to 24mg/hr).
Also applicable to VO, though Ven should not be started before Obi due to TLS risk.


our observations on the outcomes with chlorambucil and Obinutuzumab in
#CLL
- led by talented BSC med (NB) and internal medicine (IL) research student/residents. They have moved on but I want to recognize their work and acknowledge the co mentors
@drdaviddawe
@MarcGhemonc
🧵1/3

2
2
22
0
1
7

@GuiperiniMD
@tobyeyre82
Agree! This is exactly what we are currently preparing in the upcoming RT2 trial (starting in ~2025):
Pirto+Epco versus R-CHOP in 1L RT.
#gcllsg
3
0
7
Multiple COVID-19 vaccine doses in CLL and MBL improve immune responses with progressive and high seroconversion

0
2
6
We are grateful to patients&caregiver for the trust in our work. We thank our supporters at BeiGene and
@dfg_public
for providing study drugs+funding. Many thanks to
@SaheliSadanand
&editorial team& reviewers for the guidance through a meticulous and efficient review of our work.
0
0
5
🏷️Upregulation of inflammatory pathways and resistance markers such as ABCB1 were associated with poorer MRD response to BCL2 inhibition, suggesting possible biological vulnerabilities that could be leveraged to improve treatment efficacy and outcomes of patients with CLL.
1
0
6
📊Also on a gene set level, enrichment of oncogenic pathways+inflammatory signalling was observed at relapse, incl cellular proliferation. A leading-edge analysis indicated 45 diff expr genes, incl RNA splicing factors like SRSF1 and SRSF2 and apoptotic regulators like MCL1.

1
0
6
@AaronGoodman33
Challenge is often to get pts into remission before transplant.
@NitinJainMD
showed Nivo+Ibru results at ASH2018,
@DrMDavids
with Ven+R-EPOCH (ASCO2020). We are testing Tisleli+Zanu in RT1 study . Consider checking clonality (denovo progn > clon related)
1
0
6
📈A striking association between uMRD at end-of-treatment with survival is observed – pts with detectable MRD have a shorter PFS and OS (!):


1
0
6
📝In summary, these results suggest that in pts with prev untreated CLL, fixed-duration tx with Ven-Obi continues to lead to sustained treatment-free remissions.
#MRD
is a key prognostic parameter that is associated with PFS+OS, thereby identifying pts with high-risk disease.
1
0
5
Some similarities to MRD response vs non-response were observed when examining baseline vs relapse: Differentially ⬆️genes at relapse included CXCR5, IRF1 and EZH2, whereas BCL2L12, IL24 and MAPK10 were ⬇️ at relapse. Notably, these patterns were consistent in Ven-Obi+Clb-Obi.

1
0
5
Amazing study with stunning results -
@platten_michael
et al
@DKFZ
demonstrate feasibility and efficacy of an IDH1 targeting vaccine (3yOS 84%!).
A glimpse into the future, when truncal mut can be targeted with vaccines ahead of subclonal mut events.
0
0
5
Low IgG aren't the only issue in CLL-very nice study by Subramaniam et al
@UniklinikEssen
suggests molecular signature of neutrophils in CLL. It seems disruption of IFN signaling+CXCR4-mediated migration add to recurrent infections in CLL.
@BloodAdvances

0
0
5
Previous work by
@DietrichLab
,
@ThorstenZenz
and others had shown that the CLL transcriptome largely clusters according to IGHV status and presence of trisomy 12:

1
0
5
Brilliant DLBCL review by Laurie Sehn and
@gilles_salles
in current
@NEJM
issue - covers everything from molecular classifiers to R/R disease management | NEJM
0
3
5
We thank all patients, their relatives and all investigators. We are grateful for the support from
@dfg_public
,
#SFB1530
, Roche/Genentech and AbbVie. This was truly a
#teameffort
led by Can Zhang, Hyun Yong Jin, Sandra Robrecht,
@YanwenJiang
,
@MichaelHallek
and Kirsten Fischer.
2
0
5
@jeff_sharman
Agree Jeff, the MRD correlation might be ‘diluted’ in GLOW due to PFS events triggered by comorbidities/ibru tox.
1
0
4
BTK and BCL2 inhibitors have become a cornerstone of modern CLL tx; they were initially introduced as continuous regimens, administered until resistance or non-tolerance. Recently expertly reviewed by
@mshadman
:
1
0
4
@tobyeyre82
@DrMDavids
@anthonymatomd
@AnnaSchuh3
@CwynKate
Thanks Toby & coauthors
@BritSocHaem
, very timely & informative paper! Great job!
0
0
4
@tobyeyre82
I think Resonate2 and CLL14 have very diff pts - 2/3 in Resonate2 had CIRS<6, so they wouldn't have been eligible in CLL14 in the first place
-> rationale for CLL17
Illuminate is more comparable (although still fitter pts than CLL14) and looks different:

1
0
4
@chr_reinhardt
@DrAnasYounes
@LabWendel
@iannisaifantis1
@LabMelnick
@RZappasodi
Awesome, congrats Christian!
0
0
4
Given the severe impact of MRD response on survival, we asked which features determine whether a patient achieves uMRD or MRD+. To address this, we performed RNAseq of 405 CD19-enriched CLL samples from before start of tx and 44 at the time of first recurrence.

1
0
4
Studies like Murano and CLL14 aimed to introduce a new paradigm of targeted, fixed-duration therapy. In 2019, work led by Kirsten Fischer showed for the first time the feasibility of fixed-duration, 1-year (Ven-Obi) in the 1L setting in
#CLL14
:

1
1
4
Vitale et al
@BloodJournal
: Clinically relevant retrospective analysis of >800 CLL pts with BTKi/Bcl2i/PI3Ki treatment. All drugs improve pre-existing autoimmune cytopenia. Treatment-emergent AIC is mostly a rare and transient event (Ibru/Idela<Ven).

0
0
4
📈TP53del/mut and unmutIGHV are relevant prognostic factors, but median PFS for these groups are >4yrs and >5yrs, respectively – so even pts with high-risk disease benefit from several yrs of treatment-free remissions.


1
0
4
📊Next, we grouped pts into very deep responders (MRD <10^-6) or non-responders (MRD >10^-4):MRD+ status was particularly associated with higher expression of resistance markers like ABCB1, whereas MRD6 status was associated with higher pro-apoptotic BCL2L11 (BIM) expression.

1
0
4
7.) CLL14 is a huge team effort. Thank you to the pts & families, investigators, nurses & site staff who continue to support the study with such enthusiasm.
1
0
4
Since then, pts continue to be followed-up in CLL14. The aim is not so much to confirm superiority over Clb-Obi, which is no longer a standard of care, but rather to understand disease dynamics, survival and toxicity within Ven-Obi, whilst having a randomized CIT reference.
1
0
4
Detailed translational studies to identify predictors of response and survival are ongoing and we look forward to sharing those data soon!
1
0
3
📈This was particularly evident when looking at time-to-next-treatment (i.e. time to next leukemia tx or death): >70% of pts remain treatment-free and alive at year 5:

1
0
4
📈We continue to collect PB samples every 6 mo and subject these to NGS-based MRD testing – huge thanks to the pts and site staff for their support!
While the fraction of pts with uMRD is decreasing further (=> uMRD unequal cure), 18% of enrolled Ven-Obi pts still have uMRD:

1
0
3