

Luke
@LukeAmos__
Followers
1,192
Following
820
Media
280
Statuses
7,633
Dad. Tottenham. F2 doctor. In that order.
Joined December 2020
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Francia
• 461975 Tweets
Le Pen
• 417805 Tweets
Macron
• 404477 Tweets
The French
• 271306 Tweets
Melenchon
• 217929 Tweets
EMMANUEL
• 133821 Tweets
Vive la France
• 113660 Tweets
الاتحاد
• 100917 Tweets
Sean
• 98113 Tweets
Coco
• 92049 Tweets
Cruzeiro
• 64178 Tweets
Lucy
• 60250 Tweets
Jess
• 50695 Tweets
UK and France
• 41918 Tweets
Estevão
• 37207 Tweets
RIP France
• 36181 Tweets
Renato
• 35806 Tweets
NASCAR
• 34092 Tweets
Lola
• 33055 Tweets
Dudu
• 27116 Tweets
#ConexiónHondurasAllStars2
• 26786 Tweets
Renê
• 25121 Tweets
#NXTHeatwave
• 25057 Tweets
Rony
• 20524 Tweets
Quevedo
• 18553 Tweets
#DançaDosFamosos
• 16840 Tweets
FANDOM FURIOSO UNIDO
• 13096 Tweets
Tati
• 12449 Tweets
Ciaran
• 12347 Tweets
Rossi
• 11164 Tweets
#dilematvi
• 10867 Tweets
#Domingão
• 10338 Tweets



















Pinned Tweet

As horrific as 2020 has been in many ways, it has genuinely been the best year of my life. I’m struggling my way through 4th year of medical school, but in November we welcomed my beautiful son, Teddy, to the world 💙

4
0
143
My dad has contacted his GP for a lump on his back (probably a simple lipoma given his description of it)
He’s been given an appointment with a pharmacist
Before anyone asks this is not a dig, but isn’t this a beautiful example of inappropriate use of clinical staff?
359
600
6K
@RevolutionBars
@ninaa_ess
The fact you’ve put the xoxo at the end doesn’t make you fucking gossip girl, address your staff’s racism, not your ineptitude at answering messages
3
23
2K
Things I think a PA should never do:
- Be in theatre, we have surgeons to train.
- Hold any space on a doctor rota, holding a doctor’s bleep, receiving any kind of referral from a doctor
- Be paid a penny more than a doctor (I don’t care for how long)
22
303
2K
Imagine attending a stroke call as an SHO, going to discuss with the consultant to make a time-critical thrombolysis call, and speaking to someone without a medical degree
Only in the UK, would this ever be conceivable


24
231
1K
@Draconacticus
@fesshole
I think somewhat higher a moral high ground than someone who is pregnant by someone else 👍🏼
3
3
916
It’s September 2024, you’ve just managed to get a place at medical school, money is tight, you’ve heard you’re getting £5k maintenance loan for the entire year, whilst starting to rack up the student debt owing £9250 of tuition fees…
32
136
831

Here’s why reducing PA pay is in my opinion is needed.
It’s not just about doctors, it’s about my nurses, physios, OTs, radiographers who are all categorically underpaid.
New role of a PA comes in and pips them all, are you guys not outraged?
@olddiesel
Look at how difficult it’s proving, we’ve been on strike 10 times in 12 months and we’ve barely got a third of the way there
I think PAs entering as band 7 is not only disrespectful to doctors, but everyone else on the AfC pay ladder. Fixing doctors’ pay doesn’t fix that
3
12
80
42
175
714
I as an F2 in GP, with a medical degree, asked my supervising GP for an urgent opinion probably about every 2-3 patients.

According to the now-deleted case study, the PA held a ‘minimum’ of 27 10-minute appointments each day and asked the on-call doctor to review patients for an ‘urgent opinion’ only ‘once every two to three months’.
11
40
149
16
54
584
@DrPJJB
@DrJCraneBatman
If I’m in training to repay the nation, why am I also paying off my student loan?
Think before you speak lad
5
7
526
Hundreds of anaesthetists can’t progress in training, simply because the government has decided not to increase places despite an impending (if not already) catastrophic shortage of consultants
But yeah crack on with AAs

🚨 It's crazy that the NHS has told 350 doctors training in anaesthesia that the NHS has no job for them after 3 years training.
At the same time we have massive shortages of, you guessed it, anaesthetists. These self-defeating bottlenecks defy logic. Statement from
@RCoANews

281
4K
8K
4
334
495
PAs are by definition less qualified than doctors. It’s not offensive, bullying, picking on to say this.
Making a comparison between paramedics and doctors is in your words not ours.
An SHO is less qualified than a registrar, consultant respectively is a better analogy

35
50
478
@DRIISYD
I just don’t understand, pharmacists are an incredible resource
But assessing lumps doesn’t immediately scream to me to be where their clinical acumen lies?
11
13
477
I don’t think it’s unreasonable for a less well-trained role to take up more of the simple admin heavy tasks
Call me toxic I really don’t care

20
31
458
Please do correct me if I’m wrong, maybe I’m completely off kilter, but I think these are classical GP consultations
The staff member in question isn’t even on the surgery website, advertises himself as a pharmacist prescriber (not an ACP) on his LI profile
9
12
461
Does he have an invested interest?
A lord who is following every single update on the PA matter?
Screams of something 🐟
19
60
435
Went to call a patient from the waiting room in ED last night, there was a literal cheer from the crowd 🥲
Camaraderie between strangers in a stuffy waiting room with > 4 hour waits to be seen, filled me with a weird mix of emotions
14
17
404
So just to be clear, Jeannie Watkins is a director and part owner of PATH a PA locum agency, and at the same time sits on the PA school council?
Isn’t that in of itself a massive conflict of interest?
10
73
391
Only going up and up, surely we get to a point where the actual numerical amount is so pointless…
It’s essentially a tax on my earnings, for 30 years


34
46
393
It is sad to see departments and trusts jump to defend PAs in a way they would never respectively for their trainees

1/4 It is sad to see the very public onslaught on Physician Associates. We are a unit with a proud history of teaching, training and investing in our junior doctors at all levels. We are an
@RCSnews
accredited fellowship training centre in Robotic surgery (
@IntuitiveSurg
)
2
35
163
6
46
385
You will graduate with ~£100k of student debt, which is only cancelled 40 years later, by which time you’ll have paid back > £250k.
Your apprentice buddy has amassed ~£40-50k earnings throughout uni, and has £0 to repay.
How can anyone support this?
6
35
382
I’m quite embarrassed to admit I failed my final OSCE, re-sit incoming in June, any tips/resources?
149
10
379
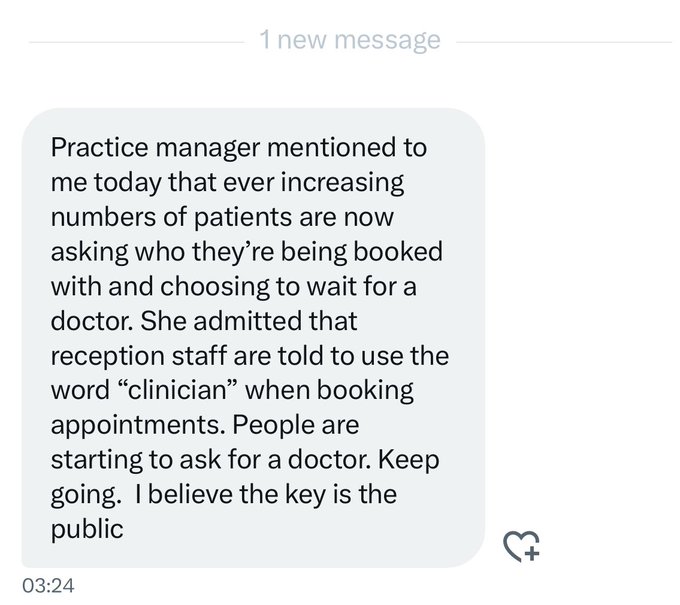
‘Clinician’ is an incredibly vague and purposeful word to mislead
Doctor, or PA, or ANP, or practice nurse, or HCA, whomever it is . Be specific to patients when telling them who they will see.
6
110
356

My dad was a house officer in 1991, his take home pay was £1500.
My F1 take-home pay in 22/23 never got above £2100.
Absolutely staggering, literally mirrors that relative drop in pay by approximately 1/4-1/3.

21
72
344
Don’t even think this is that controversial
Every single job occupied by a PA in primary could and should have been a GP trainee
How can we restrict one but free for all the other?
@jamie_wallis
Bums on seats seeing patients could also be easily sorted by expanding GP training numbers significantly
1
0
19
7
112
343
I’m a doctor, Mike. Please read the time stamps of the tweets you read.
@Iromg
Any jobs going at GB news, feel like I’d drum up the listenership given how quickly you responded to being tagged

20
17
316
Planes crash.
Let’s just put anyone behind the controls, they’ve done a bit of training but they’re not qualified pilots.

@drclairetaylor
@UKGastroDr
@NHSEngland
@RCPhysicians
@parthaskar
@DrLKVaughan
Claire. Patients have died having seen a GP. Again this is so unfair to PA’s. We make errors. Sadly patients die because we do this.
70
3
10
4
45
321
We’ve been ignored, told to keep hush hush, keep your heads down and don’t make trouble
Raising concerns, is not bullying.

I share concerns being raised about physician associates being used inappropriately to substitute, rather than support, doctors.
I’m also concerned by the toxic political debate online that is leading to bullying of PAs.
This has got to stop - on both counts.
322
172
722
3
84
292
@Niamh_F_Kielb
The word assistant is literally in HCA, you quoted ‘donkey work’ as if she said anything of the like…
The point is regarding the NA role, if anything it’s complimentary about HCAs…
1
2
279
Just found out I’ve made it through to final year of medicine, scraped it by the skin of my teeth but I don’t care one bit!
16
0
262
The money/funding/time/support is there, just not for doctors.
9 PAs hired, all 9 endoscopy trained.
Takes the royal piss.

A kind soul has forwarded my a FOI request they made to NHS England about the clinical endoscopist training programme. The replies are pretty shocking IMO. 5/


17
75
218
10
67
250
The maintenance loan doesn’t cover your rent, so you know you have to ask your parents to help, and work part time to make up the difference.
An ‘apprentice’ sits next to you, they are getting paid over £10k to do some non-clinical work outside of uni, they have no student debt.
3
17
244
If you’re an over-confident medic, you will get absolutely 💩 on.
Where are some of these PA (students) getting their attitude from?
7
14
234
Royal College of PHYSICIANS
Developed a surgical log book for PAs.
No one seems to know anything about scope, wonder what RCS would have to say about this.

23
43
232
@DrNeenaJha
Just seems to pointless to be employing people whose work has to be duplicated for it to be safe and to facilitate appropriate referrals
8
18
234
Pharmacist practitioner* sorry, is that AKA a pharmacist ACP?
Again if I’m missing the mark here, that’s absolutely fine
4
9
237
I am very aware of my inexperience in the world of GP. As an F2 I’m very up front with my patients that I’ll be discussing their case with my seniors, many consultations are left without a definitive outcome, until I confirm later
23
9
223
He does not have an advanced practice degree listed on his linked in, which I accept could be by omission, but it doesn’t scream to me to be the case
7
7
226
We need more doctors, not more people who want to be doctors.
No need for any alternative routes into medicine, given there are so many unsuccessful candidates for traditional undergrad/GEM routes
Expand medical school places, expand training posts, end rotational training
4
37
218
Imagine if we had a massive supply of doctors who wanted to be GPs, but instead we are funnelling less trained individuals into GP surgeries

in what goddamn world is calling the GP at exactly 8 am only to be in a queue with at least 50 other people already a sustainable and reasonable method towards accessing healthcare? I hate this so much
161
397
6K
3
37
216
Many conversations I’ve had with seniors (not individually critical) focus around how much they used to do in my role
Drains, LPs, lines etc…
We either have to accept that was unsafe, leave it in the past, or tackle head-on the deskilling of an entire generation of doctors
5
29
213
They have a guaranteed place at the hospital they’re training for the foundation programme, whilst you’ll be sent anywhere in the country based on a single exam (aka, random number generator).
2
18
213
Too many times, we here of the plight of the individual PA caught up in all of this.
We never here about the individual doctor having sacrificed life and limb to get to where they are, whilst simultaneously the PA waltzes in
8
27
211
It’s also nothing to do with widening participation, it’s not like these spots are being given to the absolutely defined poorest candidates in the country, how would you even go about defining that?
It’s about securing doctors, for trusts in difficult to recruit areas.
2
16
209
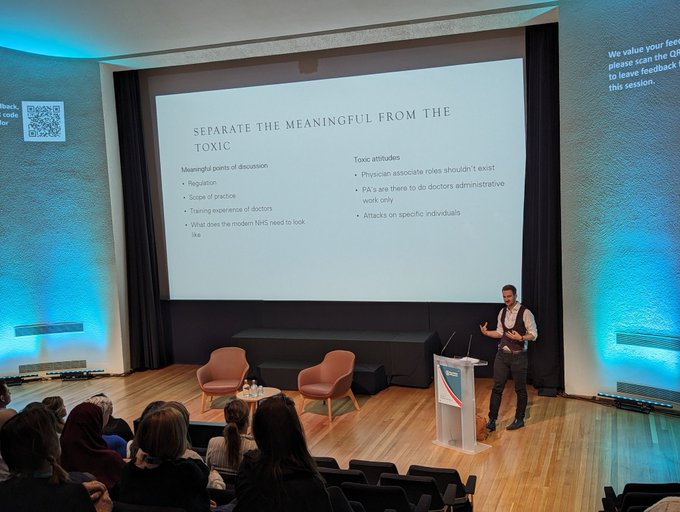
I don’t think it’s a toxic attitude to argue that PA roles shouldn’t exist
In the same time we have furthered this role; we could simply have expanded number of doctors, that really isn’t controversial nor an attack
5
29
207
You can’t see your GP, you have to scramble over appointments at an 8am rush
But there’s no guarantee that literal thousands of newly qualified GPs will be employed come August
Your government has the ability to fix this very simply, but will they?
Of the 4,000 registrars achieving their CCT over the summer, many may struggle to find work, the BMA has warned
8
70
107
6
88
210
We currently train 4,000 GPs a year, on a 3 year training programme
Imagine if we bumped that up to 5/6,000
We’d soon be able to offer thousands more appointments, and wouldn’t have to keep such a tight triage model at 8am on the dot.

Why does the UK make sick people suffer by running an 8am gauntlet through a (typically evil) receptionist just to access basic healthcare they've already paid for though?
209
845
14K
6
34
206
No admin staff on my ward or in my hospital are putting any kind of any request through.
This is not a healthcare wide thing, it’s about illegal request of irradiating imaging, by a profession that specifically are not allowed to do this.
It’s not scaremongering…

@Dr_Rajiology
A lot of admin staff put requests through on behalf of medics, at their request. They're not "making the referral". I think more information is needed about what actually happened here, it's just lazy and unprofessional to slag off a whole hospital to score anti-PA points.
6
3
10
12
35
203
Funny how quick everyone is to get out a response statement
But it’s now apparently 20 years since PAs were introduced and no definition of scope proposed by any of these relevant parties

NHS Employers has responded to newly published guidance from
@TheBMA
on the role of Medical Associate Professionals in the
#NHS
.
See the media statement from
@NHSE_Danny
:
25
5
15
4
43
197
I still find it mad any (former) doctor could ever stand as a conservative candidate, given how catastrophic they’ve continued to underfund the NHS

We are bringing your healthcare closer to home.
A Conservative Government would:
✅ Build or modernise 250 GP surgeries.
✅ Expand Pharmacy First to free up a total 20 million GP appointments.
✅ Build 50 new Community Diagnostic Centres.

800
10
59
11
12
200
Probably going to upset a few people here, but the premise that PAs have previous experience is very tenuous…
The list of accepted undergraduate degrees is huge, and in my honest opinion, a lot are not entirely, but quite irrelevant to a 2-year focused PA course

25
27
198
*Again for those in the back*
If you understood what led to the formation of the GMC, you would perhaps understand why we don’t want those who are undeniably not doctors, being registered under the regulatory body doctors set up to distinguish between doctors and non-doctors.

PA'S are being scape-goated for nunerous other issues. For the BMA union to seriously push forward that GMC regulation is not in the interests of healthcare services, shows how much power these politicians need from fear, and how future strike action will be subverted.

18
3
19
2
68
197
‘Not taking doctors jobs’
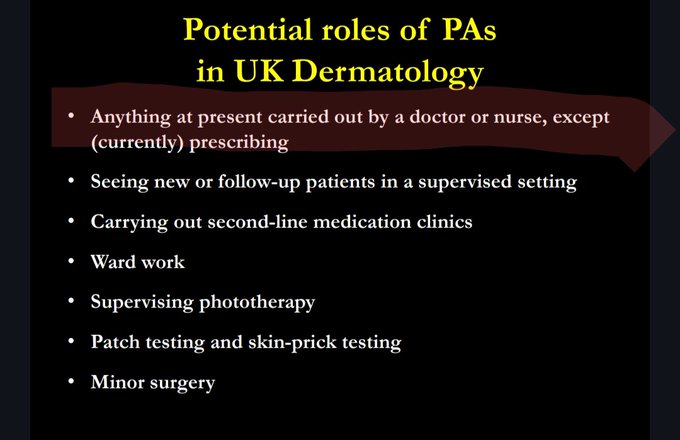
How can anyone believe this when they relentlessly won’t increase training numbers but expand PAs into incredibly competitive specialties that doctors are clawing to get into?

Huge numbers of Doctors dream of working in dermatology but are turned away due to the lack of training numbers
So it's a slap in the face to see these sorts of presentations given at the FPARCP National CPD Conference
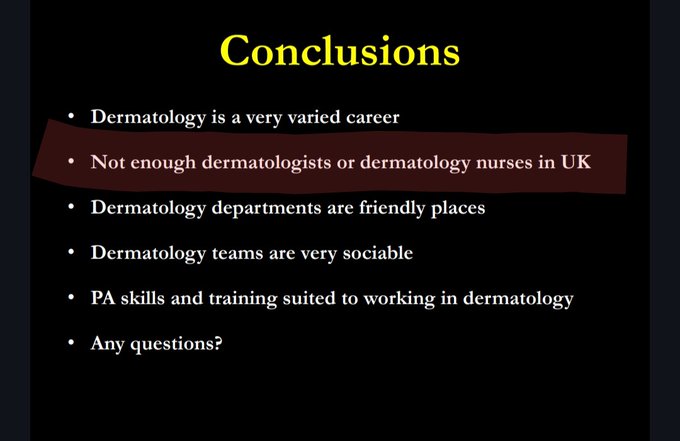
21
58
431
4
44
191
Got allocated my first choice of jobs for GP training…
Only today to be contacted by a department I’m definitely not expecting to be working in 🥲
Back to square one, admin mistakes all over the gaff
7
28
190
You’re right they represent the doctors who your incredibly new role is directly supervised by, and cannot exist without.
I’d welcome any reasonable thoughts on the actual guidance
Is the use of the word assistant your only issue? That word you literally used to go by.

You do not represent us.
Why are you writing guidance for PAs.
You have consistently belittled, undermined, disrespected, and advocated for the eradication of our profession.
Now, you draft guidance for us, still diminishing our role by referring to us as assistants.
Grow⬆️
108
9
48
4
38
188
PAs categorically should not get a seat at the table of dictating scope
Especially one that pretends to be a doctor when no one’s looking 🤡

The meta- data of the
@RCPhysicians
guidance for safe and effective practice document that has been leaked and seen by many of us suggests that Jamie Saunders (President of Faculty of PAs) may be an author of the current draft being sent around. Whether he wrote the documents or

40
210
550
6
43
190
This will always always be my response. Given PAs get paid £43k from the outset, any post created for them could have simply been a doctor, a fellowship/trainee, with virtually no difference in cost to the department/trust
Who would you rather have? I know my answer
3
17
187
Could have been at the negotiating table, chose to go on TV 👍🏼

“I very much hope they’ve had time to reflect and they're able to come back with reasonable expectations”
Health Sec
@VictoriaAtkins
says junior doctors' “unreasonable demands” are stopping a pay deal being agreed
Watch tonight ⬇️
💻 LIVE 9PM
@itvpeston
📺 1045PM
@ITV
#Peston
305
19
50
5
38
184
Everyone cries about ‘punching down’
If they’re not prepared to pay us more, then PAs should be paid less
I’ll die on this hill
6
17
180
‘Status anxiety’
I’d just rather my GPs weren’t being replaced by PAs whose only experience of general practice is a matter of weeks.
PAs should only ever supplement.
They shouldn’t be on doctors’ rotas, they shouldn’t ever hold doctors’ bleeps/take referrals from doctors.

@vinniemcdermott
@DrNeenaJha
You have status anxiety.
The NHS is desperately short of staff. We need to get some working class people into the profession instead of keeping medicine the preserve of the middle classes.
The times they are a changing.
49
0
9
4
45
179
How on earth are PAs being given ‘Flexi’ days and theatre time over doctors. I can guarantee most SHOs don’t get this level of protection for procedural time. Pathetic ladder pulling by the surgical consultant body

4
26
170
Just knew
@StGeorgesTrust
was at the centre of all this, A&E, T&O, Urology all in the spotlight over their use of PAs

@TheBMA
Despite only receiving two years’ training and being unable to prescribe, both PAs and AAs can be seen picking up similar shifts to medics, in some cases reviewing patients independently.
At 13 hospitals, doctors’ work appears interchangeable with those of associates, with the
7
121
400
7
48
173
So bold to call an assistant an assistant. People will literally take an offence to a word that’s literally in the job title
10
5
170
Why do I care about physician associate opinions about themselves?
It’s not a metric, in the bin it goes

77% (49 out of 64) PA’s who answered the question think they should work at Reg /T3 level or above. An unbelievable 10 think the should work at consistent level.


15
34
241
9
19
169
I’m 1 shift down into my F2 A&E rotation, having already done a GP job.
Seeing undifferentiated patients is so bloody difficult, it tests every last sinew.
It’s nice when you come across the more bread and butter, but even than can you be sure it’s not mouldy?

This is a Physician Associate.
They have VASTLY less training than medical students.
…Sneering and laughing at the mere suggestion that they shouldn’t see you before your doctor deems it appropriate.
For crying out loud, please
#AskForADoctor
41
186
756
10
44
164
PAs should be on an entirely different rota, in the same way as they should be on a different register to actual doctors
‘Tiered rotas’ are just a way of disguising using PAs in lieu of recruiting actual doctors
5
13
161
@Rishi17524075
This is what I’m keen to say, if I’m completely off my rocker and this is commonplace then I’ll hold my hands up and apologise
It’s just not something I’d expect
7
4
163
The job advert compares an ACP to an EM SpR
That’s the only issue that we are disagreeing with
You accept they’re not comparable roles but don’t like when we point out that they shouldn’t be compared?
Make it make sense
4
17
160
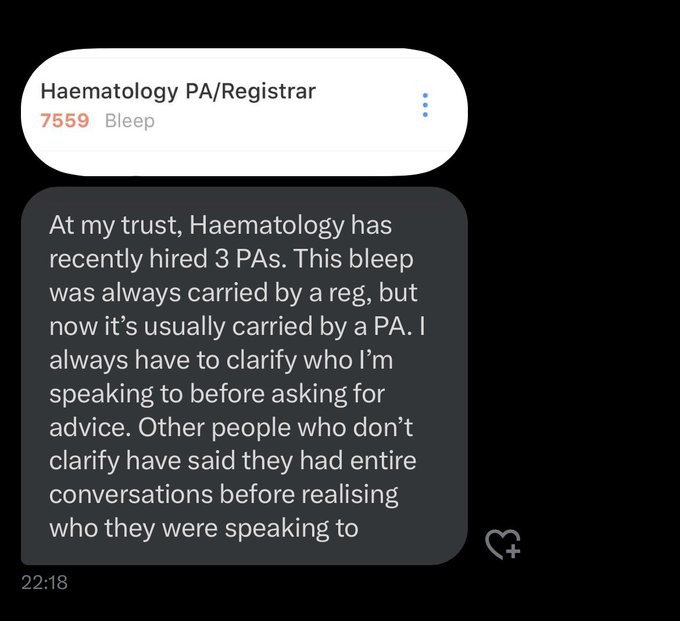
I just don’t understand.
Even the most generic ‘ward contactable’ bleeps should be held by doctors, and if not, there should be separate bleeps.
But for specialist advice? This is utter madness.

Haematology PA/Registrar
Dangerous for doctors, dangerous for patients
23
125
440
6
73
160
I’m a lowly F2, and I’m finding it tough stepping up from F1. However I don’t even think it’s an over-reaction to say it’s disgusting to even ponder equivalency between a PA and me
3
15
158
Which given the lifetime difference in financial support is easily > £300k, with no more than a handful of years of guaranteed ‘service’ to the hospital trust, really isn’t worth it.
3
13
157
It’s still absolute bollocks though? Most GP interactions are not ‘incredibly straightforward’. When is a cough and fever a simple chest infection? When is it more sinister?
‘Massive contribution’ of PA/AAs 🤐

Ooo. That’s a very selective quote. Listen to the whole thing. “When they’re complex they should be escalated”. That’s the very next line. And isn’t that the point? I regret this debate in the Lords because it denigrates the contribution of AAs and PAs, instead of celebrating
160
21
72
8
24
155
Find it really difficult to understand how any one can argue against data.
We are asking for more, because our pay has been hit the most.
We could argue all day long about who’s precise fault it is, but that doesn’t fix the problem, there’s only one thing that does.

27
40
149
@DrEilidhMaria
Often, especially unsocial hours, the F1 is one of the least well paid member of staff on site. It’s a joke.
3
14
154
I don’t understand why everyone is so precious about working ‘under’ someone else
You may work alongside (physically in space) but your role is entirely dependent on supervision by doctors, it’s not shameful to admit that
If anything it shows humility

12
22
151
All of the individual advantages PA brings to any department (purely through lack of rotation) can be brought by SAS routes/reducing enforced rotation of trainees without any of the disadvantages…
4
24
154
So your argument for PAs is some kind of anti-academic movement?
We already have something that widens variety of backgrounds to medical school
It’s called graduate-entry medicine

The problem I have with the anti-PA stuff is that I’ve never dealt with a GP who wasn’t just moving me on as quickly as possible.
Medical graduates tend to come from a fairly narrow academic background and I’m not convinced they deserve a monopoly on care.
38
4
10
7
20
151
‘I’m not taking anything from anyone else’
Well you are, because your job should essentially be another registrar, which is only not there because of orchestrated bottlenecks
Ortho PA:
‘You’ll notice this looks a lot like what a reg or fellow would do, and it is, however I’m not taking anything from the fellows or registrars’
…What about the reg or fellow that could be doing your job instead?
❌ Make it make sense ❌
14
59
231
4
43
147
Everyone loves the ‘balanced article about PAs’…
…that in no way touches upon any of our major concerns; PAs acting unsafely, those that masquerade as doctors, take shifts as doctors, hold bleeps, take referrals inappropriately…
4
36
138
I can see an argument for reducing a GP surgery’s reliance on locums.
I however would see this being done by employing more salaried GPs, not a PA.
3
15
143
In my opinion, bank PA shifts should simply not exist
You keep saying PAs are a supportive role, they should be substantive, not bank.
1
9
140
A doctor would not typically go on the reg rota for about three years
That’s how laughable this is

“A PA would not typically go on the tier two rota for about three years.”
🤯🤦🏻♂️
They should never be on the tier two rota whatsoever.
Who carries the risk when a Dr calls this team for advice, the PA issues it and the proverbial hits the fan I wonder?!🤔
30
67
414
7
21
138
@agemjourney
It’s what infuriates me the most, foundation doctors tethered to the ward
PAs? Oh come on in, let’s train you up. Let’s help you help us run clinics, you’re so helpful, what did we do before you?!
As if they couldn’t invest in their own
3
15
153
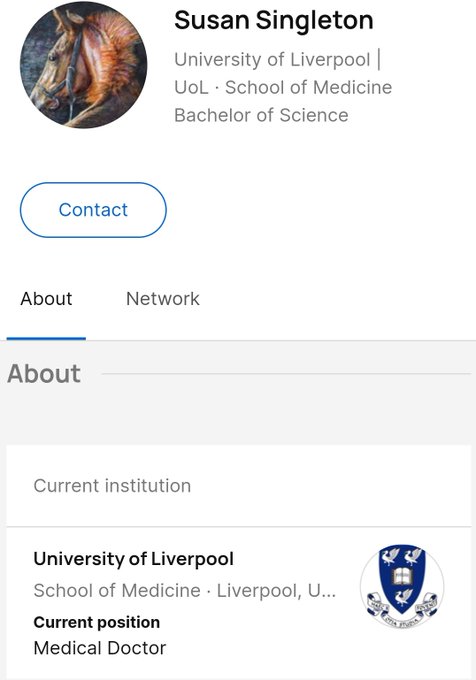
I know ideally the GMC should be involved, but when does it genuinely become a matter for the courts? It’s against the law not just GMC guidance, to impersonate a doctor
I mean... mildly amusing that you were blocked for doing medicine, by a PA whose research profile states they're a "medical doctor"
Maybe it's just jealousy?
27
27
219
7
14
135
Physician associates do not broaden a skill mix!
Whatever their previous background, is already present in…
Graduate-entry medicine!

@JayEm846
@RCPCHtweets
@dr_emmacoombe
@EmmaMDyer
@LittlePersonDoc
And this ? What was the rationale ?


12
17
57
4
31
135
Genuine question, how will regulation of PA/AAs already in employment work?
We already know that the courses they graduated from are not regulated, you can’t retrospectively just say they are now?

Regulation is changing. Legislation passed by the UK parliament means that we’re legally required to start regulating physician associates (PAs) and anaesthesia associates (AAs) from the end of this year.
Regulation will assure patients, colleagues and employers that PAs and AAs
126
39
97
8
40
132
I reviewed a patient as an F2, I’d never stopped someone’s SSRI before, I looked it up and there wasn’t an easily accessible clear cut guidance
I discussed with my supervising GP, they gave me a solid plan, now I know going forward
Most importantly I didn’t stop them overnight

8
12
132
Absolute radio silence from FPARCP on every and all concerns regarding their profession.
Interesting…
5
18
131
I work underneath my seniors, it’s not disrespectful to say that.
Why are we so obsessed with not hurting peoples’ feelings?

'They are there to work alongside doctors not instead of doctors.'
Health Secretary Victoria Atkins reiterates 'regulations' on physician associates after the death of 30-year-old Emily Chesterton.
182
136
358
6
12
130
They’re a doctor, or at least they absolutely should be, and the vast majority of the public would also expect to be seeing a doctor when referring to either of these terms

3
34
126
Who sits round the table at these idiotic meetings where they make these decisions?
Medical students, Foundation trainees, Specialty training applicants should be stakeholders in the discussions which shape the barriers put in front of us

We fundamentally disagree with the decision by the UK Health bodies to move the Specialised Foundation Programme into the PIA system from 2025 and will fight for students by resisting this change in any way that we can.
Read the full statement 👇

32
152
483
2
15
128
@DrPastry
Unless they want to spend a good 30 seconds to 2 minutes, explaining in depth their academic background leading to their title, and that they are in fact not a medical doctor (yet) to every single patient they meet,
NO.
2
5
123
Precisely the kind of nonsense that needs to be stomped out by senior DOCTORS in the departments that employ them

Oh dear me,
@NHSBartsHealth
.
Your PA in neurosurgery, identifies it has some of the sickest most vulnerable patients, purports to be working at the same level as the SHOs, is the first point of call for deteriorating patients, starts treatment and requests scans (illegally)
77
232
678
2
30
121
It’s not quite as simple as PAs replacing doctors on our rotas (although that clearly is happening)
It’s the replacement of a prospective additional doctor.
Same concept, same outcome.
@dgfull
@Cray_tweets1
@DrLindaDykes
If you just accept that you aren’t getting any more trainees, and you fill the hole with PAs, then why is there a need for more training posts?
You’ve literally solved the problem of needing more doctors in your department, with PAs.
A direct replacement.
0
6
42
3
21
122
Incredibly irrelevant
If you see a name followed by ‘GMC no. 1234 567
That’s a doctor, plain and simple. You shouldn’t have to search the register to find out they’re in fact a PA.
Transparency.

@AWJChadwick
@KeeleyMP
Wow. I’ve just noticed my mortgage reference number is also a seven digit number, calling my mortgage company immediately in case I’ve inadvertently bought a doctor!!
Dammit, I’ve just typed 7654321 into my calculator. Doctors everywhere! Aaah. I’m so confused.
#7digitscare
70
1
16
1
8
121