
Kiran Rikhraj
@KiranRikhraj
Followers
313
Following
122
Media
15
Statuses
98
Intensivist in training, Critical Care Ultrasound fellow, EM doc
Joined August 2015
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
#ConversexFourth
• 145328 Tweets
FOURTH RUN STAR
• 133355 Tweets
Osimhen
• 59771 Tweets
#宝鐘マリン生誕祭2024
• 42427 Tweets
TUBE
• 35765 Tweets
広瀬めぐみ参院議員
• 34158 Tweets
強化プログラム
• 21989 Tweets
#シャニソン水着CP
• 20232 Tweets
議員辞職
• 18397 Tweets
ナージャ
• 16028 Tweets
詐欺容疑
• 10252 Tweets


















Pearl: a failed RV is a dilated RV. One of the primary ways in which the RV compensates to stress is through dilation. A normal sized RV rules out RV failure as the primary cause of shock. Thoughts?
@ross_prager
@icmteaching
@khaycock2
@katiewiskar
#echofirst
#peoplesventricle
11
18
133
Pearl: Hyperdynamic LV does =/= hypovolemia. Keep a broad ddx - I break it down to 'low LV afterload' (sepsis, liver failure etc) vs 'low LV preload' (RV failure, tamponade, hypovolemia etc). What's your approach?
@ThinkingCC
@NephroP
@saikatmitra
@khaycock2
#POCUS
#echofirst
11
17
106
#TEXUS
? Proposing a new name for TEE guided
#VeXUS
. Calling the experts out there on what you think below!
@ArgaizR
@KalagaraHari
@ross_prager
@ThinkingCC
S < D Hepatic Vein

5
10
56
While nearing the end of the incredible Critical Care US fellowship run by
@arntfield
, I was inspired to create my first ever screencast, demonstrating the power of echo hemodynamics. Please give it a watch:
#POCUS
#hemodynamics
#CardioTwitter
#echofirst

1
11
49
#POCUS
pearl: severe valvular stenosis or regurgitation is often apparent on 2D
#echofirst
assessment. Paying attention to leaflet motion, lesions and coaptation give you big clues to severity. Pls share your examples 👇
@ross_prager
@NephroP
@khaycock2
3
7
39
The technical talk - how do you calculate VTI, stroke volume and cardiac ouput? Whether you are new to echo hemodynamics or a seasoned veteran, I hope you enjoy it. Thank you to
@arntfield
for the inspiration!
#POCUS
#echofirst
#CardioTwitter
#FOAMed

1
7
29
New video drop - Ddx of an abnormal VTI. Below I share a quick, bedside approach that I use on a daily basis and I would love to hear what you think/what you do.
#POCUS
#echofirst
#MedTwitter

0
4
20
Fun
#vexus
case in anticipation of HCP rounds tomorrow.
@ross_prager
@ArgaizR
@katiewiskar
@NephroP
1/3 Hepatic vein doppler tracing

3
2
14
If you want to want to learn about cutting edge concepts in perfusion, congestion and physiology, this is for you. Led by
#VEXUS
powerhouses
@ThinkingCC
@ross_prager
@khaycock2
@heart_lung
. Limited spots so don't miss out!

2
2
14
@KalagaraHari
@ross_prager
@icmteaching
@khaycock2
@katiewiskar
@ArgaizR
@Wilkinsonjonny
@iceman_ex
@NibrasBughrara
@NephroP
Yes. RV failure as the cause of shock requires the RV to be dilated. However, the converse isn't true. A dilated RV does not always mean that RV failure is the cause of the shock.
1
0
13

@pulmtoilet
@ThinkingCC
@NephroP
@saikatmitra
@khaycock2
Totally! VTI here is hugely helpful in distinguishing between the causes behind a hyperdynamic LV
0
0
9
'Through the TEE looking glass' - I'll be sharing some pearls and insights from a recent case at tomorrow's Canadian Acute Care US rounds. Please join below:
Meeting ID: 922 8079 7035
Passcode: 811589

Please join us Wednesday May 15th for Canadian Acute Care Ultrasound rounds.
@Buchanan_MD
, Kiran Rikhraj (UBC) and Peter Wang (UofC) will explore a variety of sonographic modalities in the acutely unwell.
#POCUS
#CCUS
#SavingLivesWithSound
@UAlberta_Sono

1
3
6
0
3
7
Mesmerising
#TEE
clip. What does this suggest about right versus left sided pressures?
Bonus: what are 5 other abnormalities in this clip?
3
2
7

Cannot wait to listen to what I know is going to be an excellent discussion by two experts in the field
@ross_prager
@ArgaizR

Its been a while in the making but I am really excited to partner with my good friend
@ArgaizR
to produce the first (of many!) Hemodynamics, Congestion, and Perfusion (HCP) rounds where we explore these topics with leaders in the field.
When: May 3rd at 12pm EST (Toronto).

18
90
249
0
2
5
@KalagaraHari
@ross_prager
@katiewiskar
@icmteaching
@khaycock2
@ArgaizR
@Wilkinsonjonny
@iceman_ex
@NibrasBughrara
@NephroP
@siddharth_dugar
@msiuba
@Jose_Diaz_Gomez
@saikatmitra05
@OKiamanesh
@iamritu
@ICUltrasonica
@ArcherKMartin
@strain_rate
@pmgjones
@pandompatam
@nathanhwaldron
Sorry to clarify - RV size alone is not a marker of dysfunction but is a key marker of one. Need a multimodal assessment to describe RV function rather than just s' as well
1
0
5
@HoosierPocus
@ThinkingCC
@NephroP
@saikatmitra
@khaycock2
Agreed re: small end diastolic volume! I find it hard to eyeball at times unless very severe. Wbu?
1
0
5

@KalagaraHari
@ArgaizR
@ross_prager
@ThinkingCC
@Sonosite
@NephroP
@iceman_ex
@nathanhwaldron
@pandompatam
@MayoAnesthesia
@ASRA_Society
@SCCM
@saikatmitra05
@ICS_updates
@MayoClinicCCM
@sono_uk
Yes I read it! Its what inspired me to do it haha
1
0
4
@kyliebaker888
Totally hear you. I tend not to use angle correct and instead manipulate my image, which is what the ASE guidelines recommend. If I cannot get a good enough angle, I will factor that limitation into my interpretation of the VTI
1
0
4

ICU Hemodynamics:
To be honest, I never spent too much time/energy in the ICU checking for fluid responsiveness (heart's ability to "significantly" increase stroke volume after a fluid bolus), but, if you still have the habit, this table from JL Teboul is a good reminder:

12
115
456
0
1
3
@ArgaizR
@NibrasBughrara
@KalagaraHari
@ThinkingCC
@NephroP
@saikatmitra
@khaycock2
@FH_Verbrugge
Love this image - breaks down the approach succinctly
0
0
4
@ThinkingCC
@saikatmitra05
@ABCDEcografia
@critconcepts
@IM_Crit_
@nickmmark
@iamritu
Ultimately, I rely on the VTI to delineate shock stages and I think
@khaycock2
said it mostly aptly - if someone is in hypovolemic shock in the ICU, the clinical picture screams of it
0
0
4
@ThinkingCC
@saikatmitra05
@ABCDEcografia
@critconcepts
@IM_Crit_
@nickmmark
@iamritu
Agree! Also 2D measurements like this are often prone to error due to off axis PLAX views. My understanding (and would appreciate correction if I'm mistaken) is that planimetry measurements of LV end diastolic area are more accurate than internal diameter measurements
1
0
4
0
0
3

@khaycock2
@ThinkingCC
@NephroP
@saikatmitra
Interesting! This is something I definitely have to read more about. Thank you for sharing!
1
0
3
1
0
3
For all the
#POCUS
folks out there,
@DeepBreatheInc
is THE AI startup to watch. Check them out👇
@ross_prager
@arntfield

At Deep Breathe we use AI to automate the interpretation of lung ultrasound, but what were its humble origins?
In this blog post we explore the humble origins of ultrasound from submarines to one of the most widely available front line diagnostic tools🚀🩺
#MedicalInnovation
0
0
4
0
0
3
@Manoj_Wickram
@ross_prager
Agree! TEE is sadly not available in all centers. I wonder if there's a way to sync the art line and EtCO2 data onto an AI-integrated defib machine that can then direct positioning changes
0
0
3
A must watch from
@ross_prager
and
@ArgaizR
!!

This Thursday!!! 🔥🔥🔥
HCP Rounds on June 6th at 4pm EST
@ross_prager
and I interview Professor Glenn Hernandez
@AndromedaShock
on assessing the microcirculation in resuscitation of shock!
Really excited for this one!
Registration:

0
15
46
0
0
2
@ross_prager
@katiewiskar
@KalagaraHari
@icmteaching
@khaycock2
@ArgaizR
@Wilkinsonjonny
@iceman_ex
@NibrasBughrara
@NephroP
Good points! However to your point
@katiewiskar
, in the cases of severe biventricular function, presumably that's the driver of shock rather than isolated RV failure. Agree with your point about being mindful how you're assessing RV dilation though
0
0
3
@ThinkingCC
@KalagaraHari
@NephroP
@saikatmitra
@khaycock2
@NibrasBughrara
I would agree that the IVC is probably not the best way to distinguish. However, I think using the VTI can tell you what type of shock your dealing with (high VTI = low afterload: low VTI = obstructive or hypovolemic in this context)
3
0
3
@khaycock2
@ThinkingCC
@NephroP
@saikatmitra
When you say Ea, are you referring to e' (diastology etc)?
3
0
3
@Rajiv_Sinanan
@NephroP
@ArgaizR
@icmteaching
@Ryan725
You have to work within the limitations of your VTI. If I get an off axis measurement, I interpret it knowing that it is likely underestimated (by how much it is hard to say) and integrate that value with the clinical picture
1
0
3
1
0
3
@norfolk_tim
@icmteaching
@ThinkingCC
@NephroP
@saikatmitra
@khaycock2
Yeah super common! Hyperdynamic systolic function and some of the highest VTIs I've gotten (35-40) were in decompensated cirrhotic patients
0
0
3
@ThinkingCC
@NibrasBughrara
@KalagaraHari
@NephroP
@saikatmitra
@khaycock2
I also find that measuring FR has a lot of caveats depending on what tool you are using to assess this. Also, FR does not mean hypovolemia eg. someone in tamponade would be FR as fluids would improve filling pressure. Thoughts?
2
0
3
Love this!
"A-lines - Straight laced. Just a normal person.
B-lines - Quirky, eccentric, and always someone to pay attention to.
Z-Lines - Quiet observer.
E-Lines - Misunderstood and anonymous."
#lungultrasound
#POCUS
#MedTwitter
#foamed
Have you ever thought about the personalities of each lung ultrasound artifact?
At Deep Breathe we do... check out our recent blog post on the core LUS artifacts and what they tell you medically.
Personality wise though...
A-lines - Straight laced.
0
3
6
0
1
3
@Rajiv_Sinanan
@NephroP
@ThinkingCC
@katiewiskar
@ArgaizR
@khaycock2
@Ryan725
@ABCDEcografia
Can't quite see the vexus well but looks like S smaller than D and some portal vein pulsatility. Regardless, what's standing out to me is whether we actually figured out why they have SOB rather than assuming it may be due to congestion.
3
0
3
@ross_prager
RV inflow outflow view, large clot in RA, RV and starting to enter proximal PA. Echogenic which suggests a subacute clot
0
0
2
@saikatmitra05
@KalagaraHari
I think S<D. D wave appears prominent and large. This would suggest congestion to me.
0
0
2
@kyliebaker888
These are circumstances where sometimes the trend in the VTI is more beneficial than the absolute number as you can test your response to interventions based on your hypothesis of why the VTI is abnormal
1
0
2
@ArgaizR
@JoseMeadeMD
@ross_prager
@katiewiskar
@NephroP
Oops sorry I should have specified! These are from different patients as
@JoseMeadeMD
said. Wanted to focus more on the interpretation individually haha.
0
0
2
@fan2physio
Nicely done! Yes the portal vein doppler does not show congestion. The loss of the waveform was respiratory motion that moved the vessel out of the field of the pulse wave doppler
0
0
0
What degree of congestion is present?
None
20
Mild
14
Severe
44
2
0
2
@iceman_ex
@ross_prager
@katiewiskar
@KalagaraHari
@icmteaching
@khaycock2
@ArgaizR
@Wilkinsonjonny
@NibrasBughrara
@NephroP
This appears to be referring to RV function as assessed by 3D echo versus semi quantitative measures such as TAPSE, s' etc. I was referring to the concept of RV dilation as a marker of a stressed/failed RV
0
0
2
@Dokutah_Vyew
@ross_prager
@NephroP
@khaycock2
Refer to
@katiewiskar
's recent post on TR! You can see on 2D that the leaflets don't meet each other during closing. Other examples would be a flail or prolapsed leaflet - that would typically indicate severe regurg
0
0
2
@Ryan725
@saikatmitra05
@EchoSoliman
@iceman_ex
@KalagaraHari
@ThinkingCC
@ArgaizR
@ross_prager
@NephroP
@khaycock2
@ABCDEcografia
@IM_Crit_
Agree with this. I find it challenging to identify which is S vs D without ECG leads and it's easy to convince yourself either way (eg. Mistaking a V wave for an A wave). ECG leads take less then 10s to apply and would highly recommend putting them on if srs about assessing HV
0
0
2

Excellent case! If you don't look, you won't know
#echofirst
#ResusTEE
ICU puzzle:
70 yo female pt without being on any medications, no smoking history, no other known comorbidity factors except moderate obesity, underwent surgical repair of hip fracture. Per note: preoperative assessment: normal lung auscultation, moderate cardiac enlargement
8
50
329
0
0
2
@ArgaizR
@ThinkingCC
@KalagaraHari
@NephroP
@saikatmitra
@khaycock2
@NibrasBughrara
I think your point highlights not to bank on the absolute VTI number because we don't necessarily know the patient's baseline. We can hypothesize based on their PMHx etc. More importantly, the VTI trend is key esp post interventions. Agree?
0
0
2
1
0
1
1
0
1
@Rajiv_Sinanan
These were clips from different patients! Sorry I should have said "fun vexus clips." But you're right - no congestion on the portal vein clip.
0
0
1
0
0
1
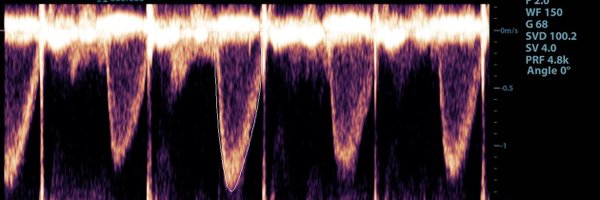
@saikatmitra05
Looks like AS and LVOTo with the dagger waveform within the larger AS waveform?
1
0
1
@alex1708ander
@saikatmitra05
@Manoj_Wickram
@KalagaraHari
Yes! RAP > LAP leading to R to L interatrial shunt. Yes to TR; no MR or AR though.
1
0
1
@Rajiv_Sinanan
Yes there was! This clip was from a patient had biventricular failure with mod MR and TR and was ++ congested.
1
0
1
1
0
1
What degree of congestion is present?
None
4
Mild
9
Severe
56
1
0
1

0
0
1
@alex1708ander
Looks like clotted blood in the pericardium by the RV. I would say regional tamponade?
0
0
1