

Sean Ninan
@sean9n
Followers
4K
Following
5K
Media
565
Statuses
21K
Actual Geriatrician. LFC. funk, disco, hiphop+onitsuka tigers. tweets about medicine+older people. Also runs a 12 CPD point frailty course @leedsfrailtyed
West Yorkshire
Joined August 2009
So my wife has been turned away and threatened with social services and a safeguarding referral at the vaccination centre for coming along with her baby. Now unsurprisingly in tears. This vaccine hesitancy amongst Asians really is a problem isn’t it?.
566
888
6K
Neurology Exam PowerPoints getting updated across the world right now.
Feel bad for Justin Bieber, hope he recovers soon. For any medical students/PACES candidate, this is a CLASSIC right CN VII palsy, with Bell's Phenomenon.


5
793
6K
@drkateflavs Complaint incoming. Softly spoken Asian lady with bolton accent is actually a formidable litigator. .
19
17
1K
Elaboration. my lovely wife was excited about her first covid jab due today and went down with our 10 month old. She is on mat leave. I'm at work. No bubbles. No nowt. Herbie is pretty chill.

17
9
834
UPDATE - Tim Hiles, Director of Ops, phoned my wife and apologised. He explained that children are allowed to be present if necessary and offered another appointment. Thank you.
10
27
577
Public Health England have just released updated guidance on diagnosing UTIs. “DONT USE DIPSTICKS IN OLDER PEOPLE” Hallelujah.

19
364
543
If a patient is walking up and down the ward like they normally do, they don’t need a physio assessment. Not everyone needs PTOT.
24
30
487
I don't want to claim staff were racist although anyone who think the experiences of an Asian woman are not affected by her ethnicity and gender lives on a different planet (where they don't hang around with many Asian women).
5
5
378
She was turned away as no children allowed. The email didn't give any details of this. She brought our firstborn for her flu jab so presumed no issue with bringing a baby in her arms.
12
10
378
“Is it dangerous if I stop this statin?”.“Not any more dangerous than being 98 already is”.
5
46
346
Vaccines will save us. Get the jab. But if we want more people to get vaccinated we have to make it easy, and we have to understand the barriers. I have spent the day thinking about what people with less money, motivation, social support, transport, time off work, would do.
5
10
318
Vaccine hesitancy is complex, and not about stupidity. I can imagine other people with less resource and motivation to get vaccinated giving up after today's experience. Hence the reference to hesitancy amongst Asians.
3
6
271
The Geriatrician's Prayer. The Courage to fight for older people unfairly written off.The Serenity to accept when things won’t get better.The Wisdom to know the difference. And The Humanity to have found out “what matters” for patient centred decisions.
8
44
283

Giving people in their last year of life calcium tablets in the morning is a great way to put them off their breakfast. How much have you reduced their fracture risk by?.
21
22
274
Do disposable aprons for medical staff have a net benefit or harm for the health of the world?.
44
43
275
It's not a small thing driving across town with a baby for a covid jab more than a year of perpetual lockdowns when your husband has spent 9 months on a covid ward and you have barely seen your own (high risk) family that you normally visit every month.
1
7
263
What is the point of doing routine 4ATs in the ED?. Most of us will miss delirium and memory problems on brief reviews if we don't do some specific testing. You might think you're good at just spotting delirium. But you're probably not. (Neither am I).
14
98
240
This pandemic and associated restrictions has been hard for us. For others much much harder. Lets make it as easy as possible to get out of this mess.
7
6
219
(Apologies for my reference to our baby as "her" baby - the patriarchy infects us all!).
2
2
198
“Progression of dementia” is a diagnosis to be used cautiously, by someone with expertise, after reversible factors have been excluded. It’s never when someone has deteriorated over a week with a creatinine of 300, a CRP of 200 and some coincidental consolidation on their x-ray.
6
17
204
So she said she wanted to take the jab. If she became incapacitated, call her husband. But if you did really need to call social services because no-one was available to look after Herbie than please do so. Because emergencies are what they are there for.
4
2
189
I'm no expert. I haven't critically appraised all this. But I have done a lot of reading on Covid-19. Check out my blog.
27
102
187
Some of geriatrics involves convincing others not to write off older people. Some of geriatrics involves convincing others not to be overzealous in investigating and treating frail older people. It’s difficult to teach (and learn!).
8
85
181
Apparently this sounded so dangerous that the supervisor thought that social services might need to be called straight away, given that there was a mother not putting the wellbeing of their child first.
4
0
173
A lot of people have replied with their own takes on things. I can be loose with words. Am about feels not deets. I started this morning reading the words of Allison Pearson talking about the stupidity of unvaccinated South Asians

4
6
170
She thought the risk from covid jabs is quite small and explained that if she did become incapacitated they could call her husband as emergency contact. Apparently that wouldn't be possible and the only thing they could do was call social services who would have to remove child.
9
5
167
I also have no desire to punish staff/get them sacked. Everyone is the hero in their own life story and this story is being told from different perspectives (although here the other side is clearly wrong!).
3
1
144
My wife is not someone who you would describe as "risky" or confrontational. .
1
0
142
She asked for an explanation and was told by supervisor the risk was of a reaction incapacitating her and necessitating a phone call to social services.
6
2
140


If your patient could wash and dress themselves two weeks ago and can’t now, they don’t need a care package, they need CGA, which may include temporary care with an aim to rehab to previous state simultaneously.
4
75
123
Has anyone done a study/QIP on NOT DOING CT head scans in older people with very severe frailty that have a fall and head injury on anticoagulations. I would be happy to do some shared decision making around avoid CT head scans but has anyone does this systematically+evaluated?.
30
15
116

She was told to book another appointment, and the supervisor walked off.
1
3
118
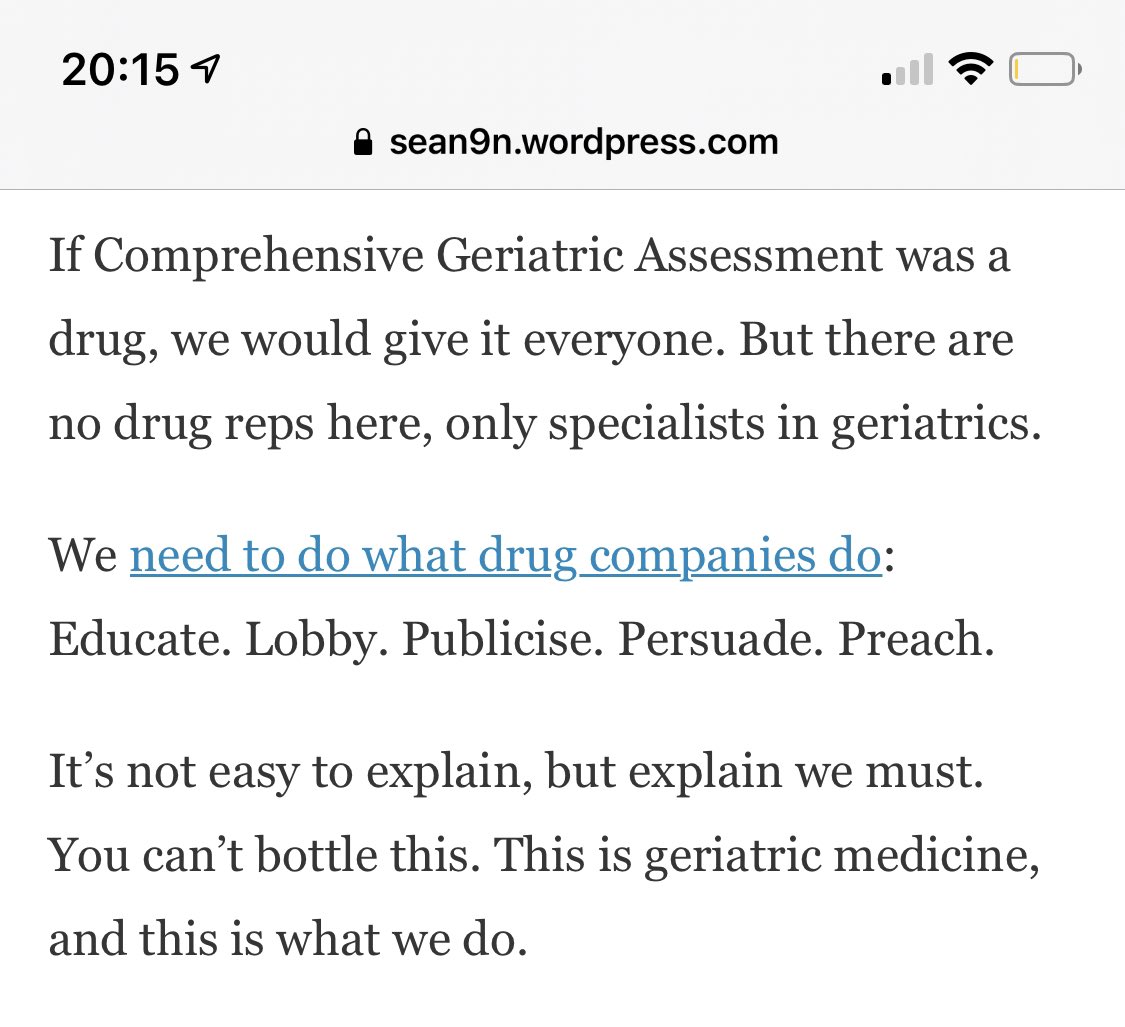
“The first line antidepressant for older people is companionship”
5
40
120
How many times are patients judged to “have capacity” when that hasn’t been properly evaluated? Why is the FY1 asked to do “a capacity assessment” on safety to discharge home when they can only see through a peephole the breadth and depth of the issues? We need to do better.
9
11
118
I tried speaking to one of my older patients about resuscitation:. “If your heart stopped beating. ”.*interrupts*.“How could my heart stop beating with you by my side?”. I think this might be the most beautiful thing anyone has ever said to me.
5
8
113
I’m a consultant and I’ve spent large parts of the day in soft play, cooking, and watching David Attenborough documentaries, with some overlap. 4 days a week at work. One day for my boys. No apologies.

I’m a GP. I don’t work Tuesdays. I dropped my kids at school, just had a tennis lesson and I’m meeting my mum shortly to take her to the cinema. All these things keep me sane. No apologies for working “part time”. #teamGP
1
1
102
Why isn’t there a CQUIN for a proper social/collateral history with activities of daily living for frail older patients? It would make a much bigger difference to quality of care than VTE or dementia CQUINs.
8
41
103
Dreams. 1. Every older person inpatient has a CFS+4AT and people understand why we do them. 2. Everybody caring for older people with frailty can describe how they normally walk vs how they currently walk. 3. Clinicians can explain the gap and understand the need for rehab.
4
31
109
You know you’re a geriatrician when your friends come round for a night out and you teach the Epley maneouvre during the predrinks.

8
0
101
Two lessons for doctors here 1) not to write off 81 year olds who may have full and active lives and 2) not all fit 81 year olds want to be “for everything.” We should still ask preferences even if we think they should be “for escalation.”.

A lovely letter in The Times reminding us of how much older generations contribute to our lives.

5
25
96
Having got cardiology advice to give DAPT to two older patients with moderate or severe frailty this week, with minor trop roses in the context of infection, this graphic is a good reminder to decision making in T2MI.

5
42
95
Positive dipstick does not equal UTI. Positive dipstick does not equal UTI. Positive dipstick does not equal UTI. Positive dipstick does not equal UTI. Positive dipstick does not equal UTI. Positive dipstick does not equal UTI. Positive dipstick does not equal UTI.

Elevated D-dimer does not equal pulmonary embolism. Elevated D-dimer does not equal pulmonary embolism. Elevated D-dimer does not equal pulmonary embolism. Elevated D-dimer does not equal pulmonary embolism.
8
17
93
Why use the CFS?. 1. CFS helps describe how older people vary .2. It’s succinct for brief handover.3. It encourages detail in taking a functional history.4. It helps set goals of care.5. It identifies the need for CGA. New video.
4
44
96
So you’ve got a case of hyponatraemia that occurred at the same time as a pneumonia but you want to stop the PPI the patients been on for 5 years? . If you want to stop the PPI stop it, but it’s probably not causing the hyponatraemia. (incidence <1 in 10,000 as per SPC).
5
9
93
So I asked my juniors to find out something interesting about their patients today. 1) one patient knows a famous local singer 2) second patient also knows that singer and worked for a tank factory 3) third patient worked for a tank factory and has met foreign leaders! Be curious.
6
10
88
“Going home tomorrow”. “How are they walking?”. “Transfers with 2”. How does that work if the patient came into hospital walking?. “Awaiting rehab bed”. “How are they walking?”. “Independently…”. (When they were previously needing help to TF). Ask about mobility. It’s crucial.
6
17
91
@DrSdeG @ShaunLintern Like other bad plans, I understood this at the beginning of the pandemic. But not allowing a triple vaccinated, asymptomatic, lateral flow negative visitor wearing the same PPE as I do, to visit their relative with dementia or delirium, seems excessively cruel now.
7
15
85
What’s really weird about this debate…we don’t want to stop seeing patients, for the reasons many have already articulated. We want systems where it’s easy to read and write patient notes. We want continuity of care. We want tests to happen without begging and chasing. 1/n.
1
16
86
I find it sad when geriatricians who stop statins due to “limited benefit” think calcium tablets are absolutely essential in the last years of life. What exactly are we trying to achieve?.

Curious witnessing a thread to see 'grown' geriatricians not batting an eyelid over making a nonagenarian with advanced dementia swallow huge calcium tablets. Oh well.
11
11
79
How many hospital trusts have “discharge wards” where patients go to wait for something - carers, intermediate care, care home etc?.
30
5
83
Great to share our trustwide plans for delirium @LeedsHospitals today. Some very important lessons around recognising the person’s capabilities before they came into hospital, the possibility for reversibility, the potential for prevention, and the power of the family/carer

6
21
79


What’s wrong with medicine? A geriatrician’s perspective. @lucypgeridoc @EileenBurns13 @mancunianmedic @Trisha_the_doc @danfurmedge @jupiterhouse1.
9
33
85
Asked juniors on covid ward what topic they wanted teaching on this week, and they said geriatrics - I kid you not. Moving from hoist to transfer to ZF+1 to walking a few yards is like following the CRP. Spread some learning man.
0
15
76
Anyway, thanks for coming. Now you're here, stay for tweets about how to make healthcare better for older people.
1
2
75
Doctors have very limited imagination when it comes to how older people function at home. It can be quite surprising how people who “look frail” can be quite independent at home, and can deteriorate rapidly when unwell and iatrogenesed. Don’t say “I don’t believe this man walked”.
3
5
73
Week 1. Delirium, AKI etc. Background of dementia. ZF around the house. Carers qds. Illnesses treated but mostly lying in bed. Not eating much. Not talking much. “Not engaging. Probable new baseline. D2A/24 hr care”.3/52 later. Eating, drinking, talking, colouring in. Walking 30m.
3
16
74
Harms of anticoagulation for AF much greater in cognitive impairment. Modest life expectancy improvement, no effect on stroke, and higher risk of bleeding in NH residents with advanced dementia. Judgement tricky!
3
27
74

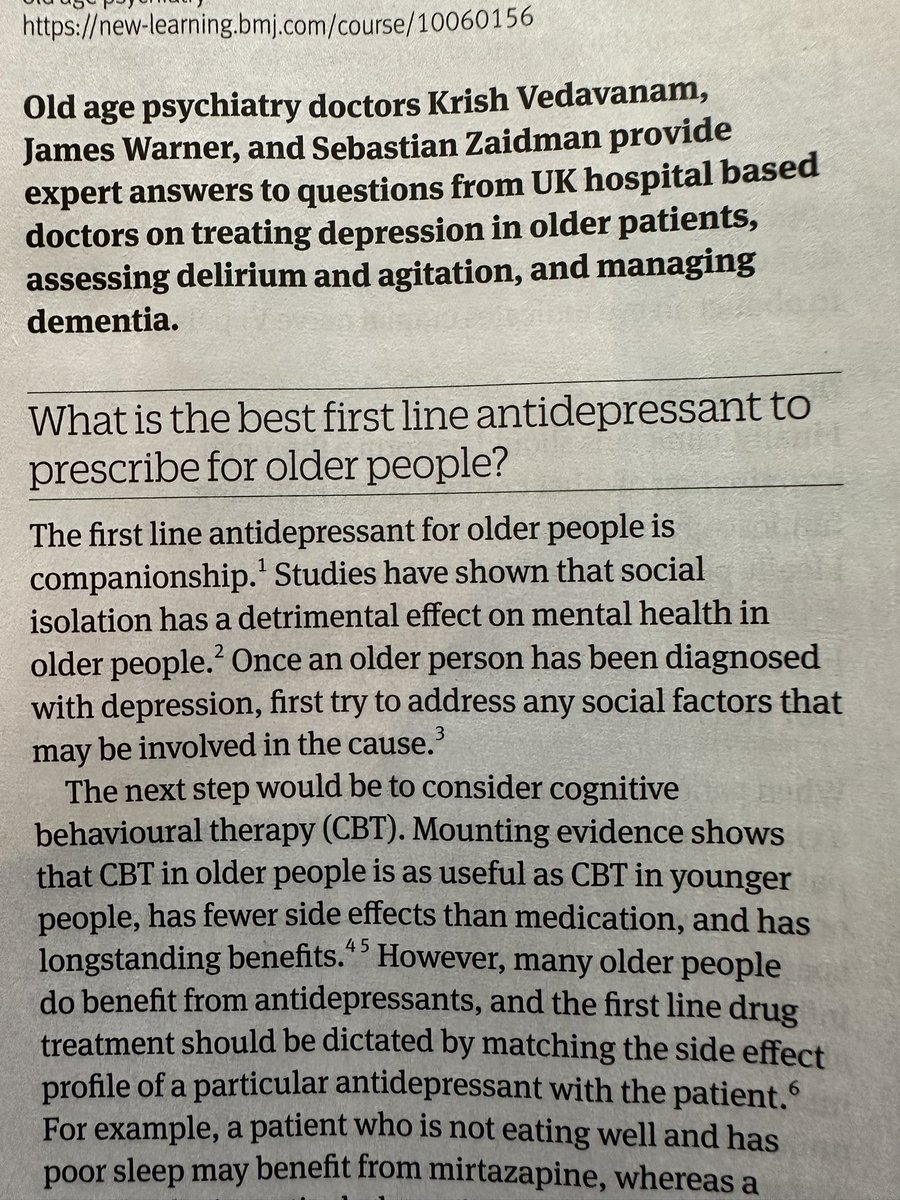
Treating older people with frailty is hard. But whether you’re in ED, Acute med, cardiology or general surgery, you need to understand the way to do it. #LeedsFrailtyEducation

0
27
74
Part of geriatrics is asking “what could we reverse here?” (e.g. infection, dehydration, constipation, retention, metabolic problems, medication harms, nutrition, deconditioning). The other part is asking “Should we reverse it?” in terms of trajectories of illness and WM2M.
7
11
68
Today, I advised a sedative, prescribed antibiotics for a UTI (no urinary symptoms) and increased chronic anti hypertensive medication. This is the opposite of what I normally do but being patient centred in geriatrics means being flexible.
4
2
72
For every patient we look after we should know how they function normally, how they function now, why there is a gap, if there is, and have a plan to address this gap in a patient centred way, knowing what matters most.
2
9
68
Asked to take a collateral history for cognitive decline. Try this

8
23
64
12 CPD points for £80? (virtual) and £120 in person. Too good to turn down! Come and learn about frailty, delirium, dementia, falls, polypharmacy and more in the wonderful city of Leeds.
4
32
63
Why do we palliate some patients straight away, but with other patients spend a long time trying to get them better? This patient looks so frail. A very good question. A) Baseline. The term seems to be unpopular.
4
15
65
Time for an annual round of 21 tips. For junior and not so junior docs looking after older people.
1
51
64

85 years old.CFS 3.4AT 12.NEWS 0.A powerful story. If you want to learn more about how useful this concise information is, and how it affects management read my blog and come along to to learn more. @LeedsFrailtyEd.
5
39
67
When we say people “look frail” we mean they look thin and unwell. This isn’t the same as frailty. All of us who are thin in old age (some of us are thin in young or middle age!) are at risk of being dismissed as frail if we come into hospital tired and unwell.
4
16
65

I’ve met a bunch of bloody lovely geriatricians in the last few weeks who give me hope that things may not be as bad as they seem. Because my colleagues are boss! Choose Leeds. Choose Gerizzzz.
3
4
60
20-30% of patients in hospital have delirium. Many are missed so we need to sceeen - using a 4AT. prevention is better than cure. We need to systematise good care for patients at risk of delirium. Here’s what to do . @LeedsFrailtyEd.
0
29
61
Forgot my stethoscope on a home visit. Luckily the patient had one for me! A vintage number

6
2
61
“They’re for full escalation”.But what if they don’t want to be?.Even where I would offer resus, many of my patients (mostly >80, mostly at least moderate frailty, but a fair few mildly frail or not frail) don’t want to be.The most common reason I record a DNACPR is pt choice.
11
5
58
“Orientated TPP” “compos mentis” unhelpful terms. A 4AT score of >0 doubles your length of stay. You’ll miss some patients with memory issues with superficial chats on ward rounds. It’s not normal to not know your age or what year we are on. Do a 4AT.
0
25
60
How to diagnose UTI in older people. Thoughts?.Might have to pinch and zoom on a phone

14
18
61
Lesson of the week. If an older person who normally lives independently presents to hospital unable to explain why there are or what happened, assume delirium even with normal obs and looking ok. In this case bloods revealed AKI and raised inflammatory markers. no conincidence.
1
18
57
Why am I not convinced that a mass transfer to residential care is the answer. ?.
5
4
55
If you’re a clinician looking after older people in ED or specialty ward? If you’re in primary care doing frailty work but want to learn? If you’re an MDT member doing one part of CGA but wants to find out about the whole? If you’re wondering what the point of CFS, 4AT etc is?👇🏾.
12 CPD points for £80? (virtual) and £120 in person. Too good to turn down! Come and learn about frailty, delirium, dementia, falls, polypharmacy and more in the wonderful city of Leeds.
2
32
52
Why is the NHS less productive? Why are doctors so unhappy? could we fix both these things? With warnings from @ShaunLintern and lessons from @Philippa_Perry @danariely . @Thea_Stein @parthaskar @drohanlon @mgtmccartney @mellojonny.
4
20
51
There are *some* patients who present to hospital with a very clear history of dementia who should just be diagnosed.

Services need to consider how best to identify and diagnose cognitive impairment/dementia at the time of admission for fragility fractures #BGSconf

2
16
53
Give me strength. The strength to fight for rehabilitation for older people, the courage to address when medical care won’t work, and the wisdom to know the difference.
2
8
55
4. Everyone with delirium gets a basic PINCH ME. People get it like they get sepsis. it’s more common…. 5. People take the time to find out WM2M. These aren’t geriatric medicine things, they’re older person things. And that means they’re most of the hospital things.
4
14
56
How many geriatricians think a blood pressure of 120 is “good” for severely frail older people in last couple of years of life? Of course it depends but we are wedded to a model for younger people. “Allow BP 160-170” is something I often write as a manager plan esp if falls.
Older people remain on blood pressure agents despite being hypotensive resulting in increased mortality and hospital admission
7
7
53
We don’t need to bring back nonagerian care home residents for follow up chest x-rays every time. Are you actually worried about cancer? Are they? This is not the population to enforce screening on.
5
9
52
They tried to make me go to rehab, I said.Yes, ideally in my own home, to judge my "rehab potential".But if not, a rehab bed to roam, with CGA credentials. Not a night assessment in an enhanced care bay.Or a one way ticket in D2A. (Unfinished).
2
5
52