

Dan Furmedge
@danfurmedge
Followers
6K
Following
12K
Media
356
Statuses
11K
internist/geriatrician/pragmatic educationalist/consultant physician @gsttnhs Censor @rcphysicians IMT TPD sensible medicine/SDM/QoL/EOLC. 👀 for squash buddies
London + Portsmouth
Joined August 2012
Things I don’t want to change after COVID:.- the lifts are working efficiently .- great team spirit and enthusiasm .- whole of medicine comes together daily .- get to meet to and chat with lots of consultants in other specialties .- lots of red tape gone to get shit done.
25
142
1K
This weekend the St Thomas’ medical consultants on call are me, and one of my best friends that I met on the first day of university in halls. We still can’t quite fathom how it happened or who let it. 😂.
8
5
793
So we have a lady who was NBM for ages, now after a long time and lots of work from the SLT team she can have a normal diet and fluids. She says she has never had champagne. Guess what we are having on the ward round tomorrow? 🍾🥂.
16
61
745
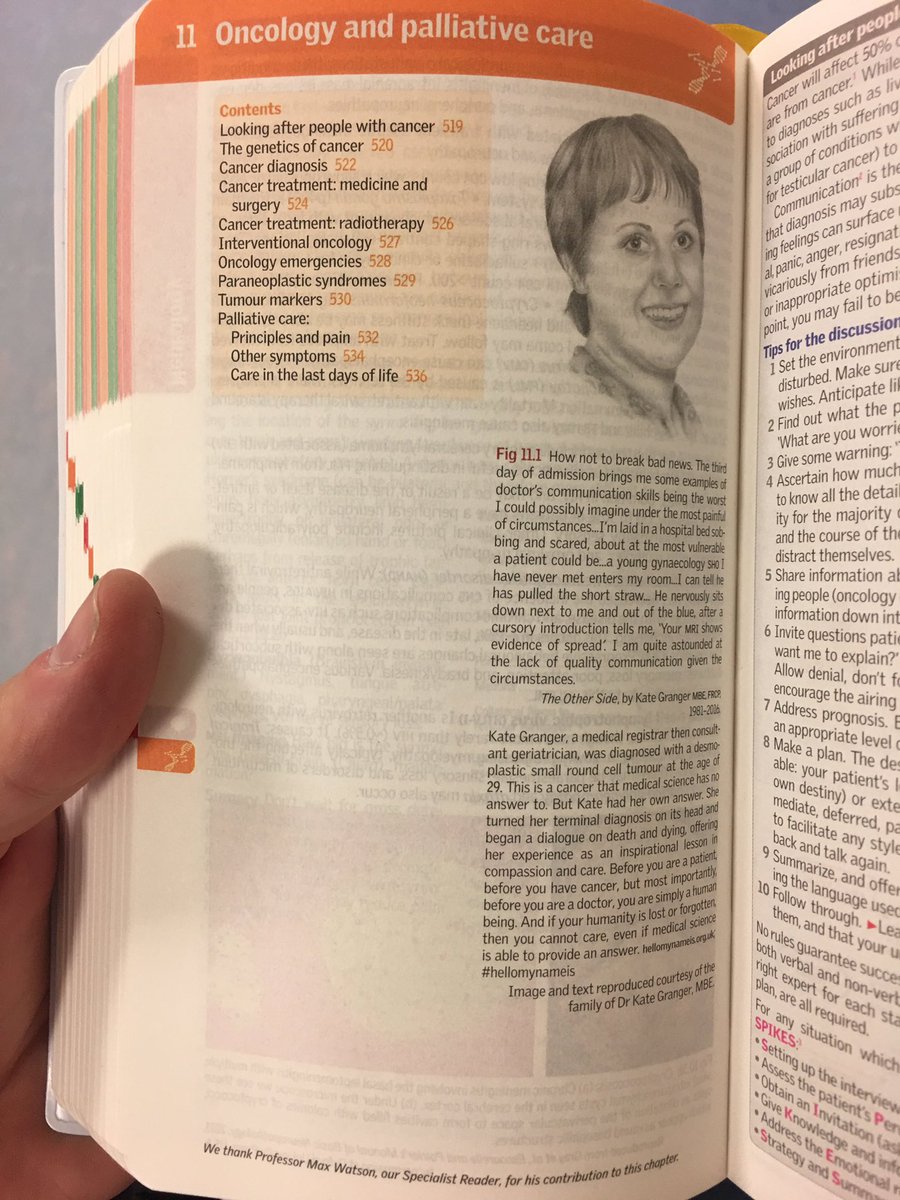
Great to see @GrangerKate's legacy living on in the brand new 10th edition of the Oxford Handbook of Clinical Medicine. @PointonChris
3
240
663
Here we go, night 5/5 covering #JuniorDoctorsStrike . Definitely don’t want to be here again in a month. Forgot how antisocial nights can be - luckily with a great bunch of consulrant colleagues in medicine and ED . Please sort it out @SteveBarclay @RishiSunak

24
84
651
My kind and gentle Grandad has just died, at home, symptom free, with family thanks to frank discussions, an advance care plan and a great community nursing team. Has given me personal experience of how important is. Particular thanks @HurdJo for your support to my grandparents.




50
69
620
Really wish I was one of those old school consultants with a massive house and garden who has everyone round for a summer BBQ/party. Would love to do once this is all over. Sadly my 1 bed flat probably ain’t gonna cut it. Will keep playing the lottery 🤞🏻.
42
10
599
Being contacted by a genuinely distressing number of outstanding doctors who cannot find FY3/4 posts and are unemployed from August. First year I’ve noticed anything like this. Concerning. What can we do?.
26
153
519
I am fed up of the relentless focus on internal delays, earlier discharge, AM discharge. We already have SDEC, hot clinic, hospital at home. Minimal gains to be made. Why not sorting root of issue? Social care. Therapy. Stepdown beds. Care home beds. Proactive community care?.
8
77
499
The 1st nights were novelty. Now starting 1 of 5 night shifts to support doctors industrial action. Not looking forward. I’ll say it again, if this keeps happening, will be a lot more expensive than just agreeing a sensible pay rise. @SteveBarclay @RishiSunak.
12
89
493
Today I watched 10 doctors try to have a DNACPR discussion in the context of discussing a deteriorating patient. Even those most skilled in communication made the task so much more difficult that it needed to be. @DrLindaDykes we need to sort this out . ⬇️.
41
139
435
😣 Fever, sore throat. Looks like it’s got me guys. Feel well atm. Main thing am gutted I can’t help the team at work with the mega stuff they have to get in place this week, in including acute take, doctor redeployment, care home planning. Good luck team see you in a week!.
78
8
419
My old F1 left after F1 UK, is 1yr resident in USA. <6m in she does more than IMT3s. Works hard/long but has advanced 3 years in 6m. Never does admin, bloods - people for that. Teaching culture and time embedded. Says it’s not down to luck or individuals whether you learn.
7
42
438
@Jeremy_Hunt You are a lying, spinning, horror of a health secretary. You don't realise whole country is behind us. They won't forget.
18
146
378
Been told in our trust that we may need to cover large numbers of locums as COVID19 takes off. But if i do this i will end up paying more than i earn in pension tax. @MattHancock this may be a national emergency, please suspend tax rules immediately so i and colleagues can help.
16
121
411
Just totting up how much it will cost just general medicine to cover the junior doctor strikes next month at our hospital alone. Honestly @SteveBarclay just put a sensible offer on the table. It’ll probably be a lot cheaper in the long run.
13
51
355
If the Nightingale in London is to be reopened at all as a step down/rehab/medically stable bed base I sincerely hope that this time round they get a geriatrician in.
12
15
352
Here he is, Bill “the bed” Addison says hello to you all and says he is too old for social media but looked sort of pleased to have been mentioned! Massive @GSTTnhs hero for many years for anyone who has worked at St Thomas!. @mancunianmedic @TYoungstein @b_modarai @Pinkywyatt1

19
14
330
About to do a year 2 MBBS lecture. There are 500 students in a year. Looks like <30 have shown up in the preceding lecture. I know it’s all adult learning and can watch online. But seriously? I’m not going to bother next year if you can’t be bothered to come.
80
16
344
Judging by the medical take this weekend, we are returning to usual - have seen core presentations in geriatrics, cardiology, respiratory, haematology, gastroenterology, neurology, stroke, toxicology (+++), nephrology, oncology. And just a couple of ?COVID.
9
32
343
Friend has text me with a knee swelling. Obviously a simple bursitis. 111 asked him to attend ED. No wonder ED is fucked. Honestly.
30
10
333
Seen in the notes:. 2/7 SOB.O/e crackles, widespread wheeze . Plan.D-dimer .?CTPA .Salbutamol neb. We are losing the plot. Clinical thinking, problem solving, interpreting history and signs. Need to sort out how we train people to think in medicine.
51
23
325
Absolutely outrageous and frankly disgusting. I will be writing to Chair of NMC again. THIS is how nurses will be scared into doing the wrong thing. Because they fear for their registration. Appalling.

Latest from our legal expert on CPR: nurses must start resuscitation if there's no DNAR notice, despite what best practice guidance says. Read his professional view on recent NMC case
23
88
314
Consultants, once again, encourage encourage encourage everyone to use your first name. It’s no longer 1951.

31% of medical trainees address consultants by first names despite 76% believing those they addressed by first names were more approachable. Do you think this impacts likelihood of raising concerns, staff wellbeing, recruitment and staff satisfaction?.
62
35
284
@SarahMillican75 working. Because unlike Jeremy H would have you believe, we all work weekends!

12
149
272
Last night, paying for some drinks with my NatWest debit card from what is still technically a NatWest student account. Spotted one of the new F1s buying theirs with a gold American Express card. Wondering where did my life go so wrong? 😂😂.
16
5
279
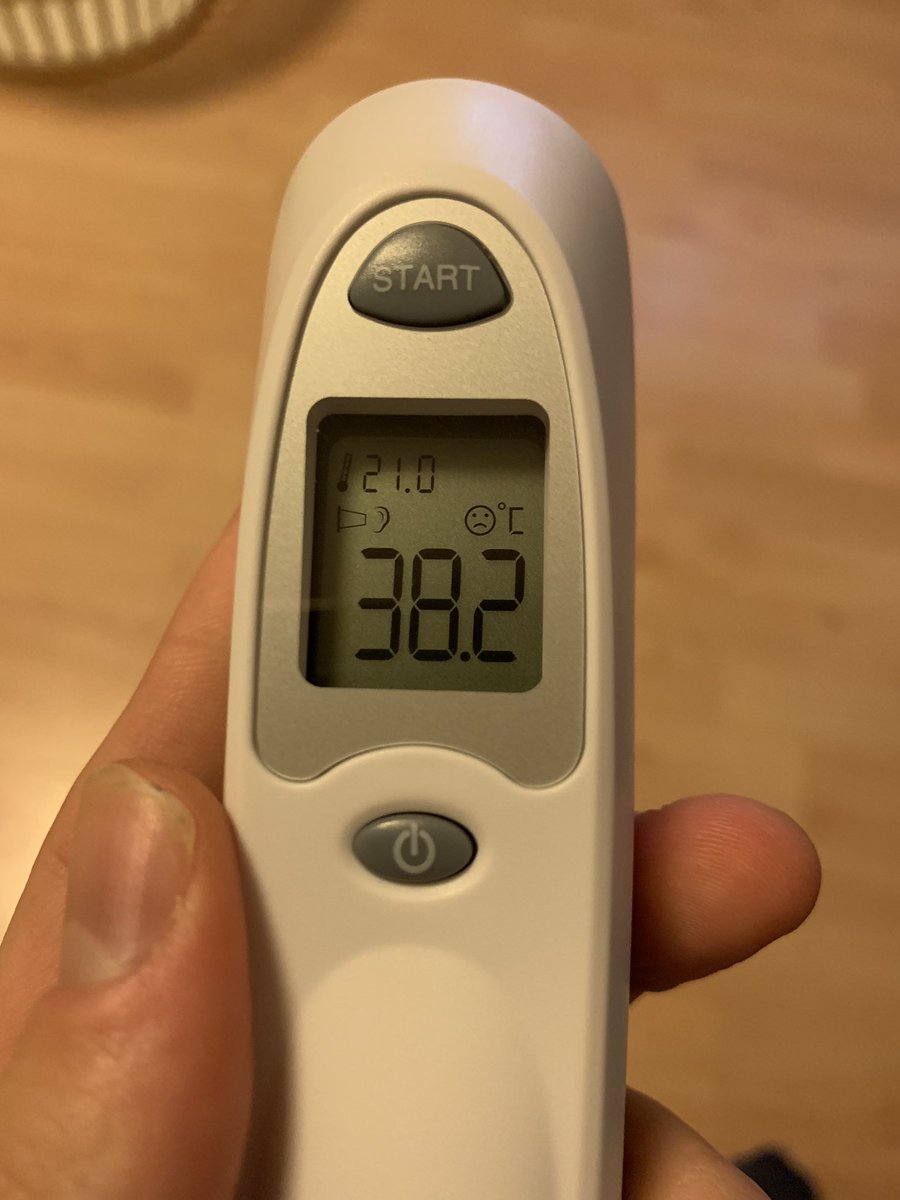
Pulse of 110 and temperature of over 38. However in the context of severe coryzal symptoms and generalized malaise, my own clinical judgment tells me I do not need IV antibiotics, a lactate or a catheter. #notalwayssepsis #useclinicaljudgement
27
38
278
Medical consultants right now falling into 2 categories . 😎 Med Reg vibes reactivated . 🫣 Checks booked AL on strike dates.
7
5
265
UK citizen born here, until A-levels. Moved to Oz for uni MBBS. Worked in Oz 3y as dr. Completed FY1/2 equiv. Had to return to UK pers reasons. @Sydney_Uni MBBS NOT RECOGNISED. Can’t work.Has to do PLAB.6 months part 1 wait .Now 6m part 2 wait. 12 months. WTAF @gmcuk WTAF.
32
28
261
Omicron can be renamed the silver wave. Little respiratory illness but lots and lots of frail older folk with falls, delirium, functional decline needing geriatricians, PT/OT/SS and care home beds and we have nowhere near enough. Really exacerbates a long standing problem.
6
73
260
Have worked >80 hours this week due to normal on call and strike cover. V lucky to be on with this bunch of awesome medical consultant colleagues covering acute/general/geriatric med @GSTTnhs and providing support to ED. We’ve managed to find half an hour to grab lunch together!

14
13
256
Again on take today, 3 patients with advanced cancer. None had ever been given a prognosis or a chance to discuss TEP/resus status or prognosis. All had thought deeply about it and knew exactly what they wanted but hadn’t been given the chance to say. FFS #havetheconversation.
18
66
248
I once phone the GOLD director on call at night as SpR due to an extremely unsafe environment. They refused to talk to me and asked the general manager on call to speak to me. I was told “this is just how it is round here”. #IamHadiza #bawagarba.
20
163
238
When we do our mortality review in geriatric medicine, by far the most common question is:. Did we do too much for too long/should we have considered palliative/end of life care earlier?. Yes this seems so hard for so many doctors.
19
81
231
Don’t delete the on site gym and squash courts etc. and pretend the NHS is bothered about well-being . Don’t cripple us with pensions tax. Don’t continue the real terms pay cuts. Don’t fuck up recruitment for junior doctors to specialty training. ….

Minister ‘not sure what more we can do’ for NHS staff as MP's described burnout ‘emergency’
4
37
241
Today I completed “fast track” paperwork for a patient to move to a nursing home who is rapidly approaching end of life. Documents submitted by email to CCG. Message back. We are unable to accept these-need written signature then rescan and send back. Give me fucking strength.
34
61
222
Just voted in favour of a move to support assisted dying. It would need extremely robust safeguards. But I believe that in some circumstances, people should be allowed to choose when they die. Palliative care can be amazing cannot solve the deep issues for everyone.
17
24
195
I am 5 years in. If I have this similar bill my savings will be wiped (and more) and I will leave for Australia where I have been offered a job for 3x my current salary with much better working conditions.
7
43
194
Can anyone explain why the London weighting for doctors remains about £5-7k lower than other NHS professionals and hasn’t changed since its introduction in the early 2000s?.
16
16
189
Very satisfying weekend in the Acute Older Persons Unit this weekend:. 19 patients seen.15 home, many w community services .2 admitted .2 aiming for discharge tomorrow. Services used:.H@home team.Rapid response.RH carers.Families.Rapid geriatric HOT clinics.Old age psych. ☺️.
13
43
193
Just added up everything I do at work currently and it adds up to 17 PAs 😱 for which I get paid 12 and that doesn’t include all the PACES and RCP committees and other extra bits. Time to drop some stuff and get a life 😂.
13
0
194

@RowansHospice @RobertIger we hear you are the only one who can make this happen. Someone dying, won’t make release on 20th Dec. Wants to see the new Star Wars before he dies. can you help?.
2
16
181
Something that upsets me most is relentlessly pursuing tissue diagnosis and delaying decision making in b frail new cancer pts, giving hope to families, whilst patient doing downhill when clear they will never be suitable for treatment. Geriatricians we need to step up here.
16
16
173
A lady undergoing non-curative Rx for metastatic cancer. A man with advanced cardiorenal disease. A nonogenerian with multiple comorbdities. None with #DNACPR discussions despite many opportunities. All were happy to discuss and plan on PTWR tonight. #havetheconversation.
7
48
169
Hi .@Jeremy_Hunt we have no beds, 20 patients in ED waiting for beds and more coming and it's the same in every hospital in UK. .
27
319
165
Just a reminder that a high CRP does not always need admission. Young people tolerate infection well, are usually sensible, will take abx and will come back. Can share any risk with them. Have sent a 40F home before with a CRP 544. She got better with oral abx.
22
30
168
Once again I am asking who on earth is running the Foundation Programme in the UK?. Doctors with no posts, trusts forced to fund new posts with no money, now doctors told some allocations wrong. Shower of shit. Wish I was not surprised.
3
20
175
We are not teaching Medical SpRs to be take consultant. They are too busy on calls, coordinating and clerking. Then suddenly as Consultant, have to review all the patients on the take. Completely different skill. Senior Medical SpRs need to do the PTWR themselves. Before CCT.
18
33
158
I have seen a lot of COVID in the last 10 months, but when someone you know dies at 55 from it after a very rapid illness it suddenly seems all the more real and the worry for other family members increases. Thank you to @QAHospitalNews @icu_portsmouth for looking after her.
28
11
162
1 Delirium secondary to UTI.2 Asymptomatic covid-19 +ve . Obviously the evidence for UTI was 1+ leukocyte on a urine dip and no other symptoms . 🤦🏼♂️😑😭🙉🤡🤬.
15
6
170
Some thoughts after a week on AMU and recent examining PACES. If we focused on proper teaching (inc. consultants) in following areas we could avoid a lot of unnecessary tests and admissions:.1. Syncope.2. Troponin.3. Acute headache.4. Accepting and managing risk.5. TIA.
16
20
158
To all my consultant colleagues who are doing ward and have a new team since August:. Have you taken your new team for coffee yet? If not why not?. Have you done a reverse ward round yet? INWN?. Have you proactively done a CBD/ACAT/MiniCEX yes? INWN?.
15
15
161
And thank you again to his carers, who have just turned up having heard he has died, and cried and consoled my grandmother, then offered to clean him. 🙏🏻.
My kind and gentle Grandad has just died, at home, symptom free, with family thanks to frank discussions, an advance care plan and a great community nursing team. Has given me personal experience of how important is. Particular thanks @HurdJo for your support to my grandparents.
8
15
157
My letter to .@damejanetfinch Chair of .@nmcnews about the caution given to nurse who did not do CPR on a clearly dead frail nursing home pt

24
83
153
How I record my reflections in my eportfolio ever since that awful legal case where a reflection was used against a trainee.

11
66
148
Brother texts at 1400 to say he thinks my stepdad is having a heart attack. Less than 3 hours later he is sat on CCU, 2 stents in place and cracking a joke cos he feels much better. Great work and thanks to @SCAS999 and @QAHospitalNews. cc @MCubbonNHS.
4
19
139
I work in a large teaching hospital and rarely see a medical student. We have set them up to fail. No apprenticeship. Poorly considered curriculum designed (at KCL anyway). No real longitudinal time with clinical teams. Constant interruptions. No “on call” experience.

Interesting conversation with a medical student:. 'They don't teach us enough to reason from first principles. I know there is stuff they are leaving out. It's all about the guidelines.'. Yeah. And paying through the nose for it. ☹️.
13
14
149
Stop filling in then sending me your own SLEs 😩. “Good presentation”.“Remember to do x”. I’m supposed to write the feedback not you. Is it that bad that we expect trainees to fill their own feedback cos they know consultants won’t do it?. If it is then the system isnt working.
47
6
150
Yesterday - inpatient covid ward .Today - hospital at home (lots of covid).Tomorrow and Sunday - acute medical take (lots more covid. ). Life of a geriatrician . Happy New Year!

11
3
146
Well this has maybe backfired! Looks like am going to have to be night medical reg 24/25/26 😂.
Hoping that I will be “needed” at work at some point as 5 festive days alone in my flat now I can’t go home which includes Christmas, my birthday and New Years doesn’t sound that fun! 😂😭.
19
3
147
Fully supportive of the thought to increase and honour medical school places BUT there would need to be a commitment to providing additional Foundation Programme (and beyond) posts for these doctors in 5-6 years time. @MattHancock.
6
16
138
@timricketts_ That frail older people usually can’t come back to bloody outpatients. Just see them as an inpatient and let’s make a sensible plan which avoids them waiting for transport for hours and being stretchered into hospital having just been discharged from a long stay a few weeks ago!.
0
3
139
For anyone who hasnt done one a reverse ward round is great .- junior doctor gets to run the show with feedback.- consultant gets chance to a) write notes how they like it and b) review other stuff and think at the same tine.Obviously need to pick your times but highly recommend.
11
24
129
Sorry but I’m afraid I just have to share how cute my 6 month old niece is 1/2 😍
10
1
124
.@Jeremy_Hunt came to my hospital today and had to be hidden and flanked by multiple police. If thats what he needs as the boss says it all.
10
124
121
Wow. Of those ventilated for covid-19 just 13% 71-80 and 6% 80+ survived. Remember these are those selected as candidates for ventilation. And if you arrest with covid 0-1% survival at any age, slightly higher if young and arrest on an ICU. Remember to #havetheconversation

6
56
126
Well. I’ve seen 50 patients on the medical take today from 0800-2030. Was working with an amazingly efficient clerking and acute medicine unit team. Now my brain has slowed to a dawdle I am going to sleep. 😂😴.
5
1
127
1. If a patient is likely to die say it. They are probably going to die. Stop using eupehmisms because tou think that you are being gentle or kind. Youre not. Patient/NOk doesnt know what you mean by very poor prognosis. Be honest. Even if there is a 20% chance of death, say it.
3
13
115
To the orthopaedic SpR who just asked my team “why are we even bothering” to as you about management of our 81 year old’s wrist bone fracture. I don’t quite know what to say. Apart from have you seen Mary Berry?.
11
19
117
Despite the psychological doom I now remember at the start of 4 night shifts, I head in to the first tonight, thinking I will do this time and time again if needed. Nobody starting medicine 10-15 years ago could have predicted the stall in pay this government has created.

2
2
110
Current world heros are #anonymous taking down Russian government websites and playing Ukrainian music and war scenes on all national Russian TV challenge to counter the propaganda there and much more. Outstanding. 🇺🇦.
0
24
102
This is a true CFS of 1 in a 90 year old @drvabennett.

Japan's oldest fitness trainer is a woman in her 90s and she has no intention of stopping before she turns 100 🏋️♀ . via @dw_arabic
6
17
109
Did a ward round today. 8 patients 'for CPR'. When asked, 7 did not agree with CPR. 4 vehemently so. Doctors must stop assuming.
13
67
100
So anyone want to form a group to retrospectively review GMC MPTS outcomes in the last year? Would be interesting to review and publish outcomes compared to what jobbing doctors think is right. And perhaps could do a patient arm too to see what they think. What a mess.
22
7
102
Off to bed. Feel fine. Mild fever only real symptom so this could be any old viral lurgy. Wish I could test. Thanks all for well wishes and offers of help! Feel like fraud as feel OK!. Lots of good chat and sharing resources with other community docs today today. Good luck all.
19
2
104
Hoping that I will be “needed” at work at some point as 5 festive days alone in my flat now I can’t go home which includes Christmas, my birthday and New Years doesn’t sound that fun! 😂😭.
19
0
107
Pneumonia is often a last illness in frail older patients. Recognise this, be explicit with juniors/patients/NOK about risk of deterioration/death, set expectations and if patients do well, think about further discussions about the future. #BGSconf.
4
38
99
Sad when the F2 you are on take with tells you that this was the first time anyone had ever observed her interacting with a patient as a doctor and given feedback. Why are we still not getting this right?.
10
15
104
Love that we are being annexed by the world - the strain has been going round since September, you’ve all got it, you just haven’t spotted it yet. Except Australia and Denmark cos they are also excellent gene sequencers.
5
12
102
Getting pretty fucked off with the system trapping people in hospital. Feel so helpless to move them on. Particularly those with behavioural issues, so much worse in hospital who apparently fall in that limbo land between mental health, medicine, and social care services.
6
14
104
So those in favour of first names of consultants for the rest of the health team esp junior doctors:.- almost all junior doctors.- allied health professionals.- many consultants . Those against or who feel their ego requires being called doctor .- a few consultants . 🤷🏻♂️🔥.
26
5
101
We just got EPIC. Promised an intuitive amazing system. We will get there and it will be OK but absolutely not impressed. Awful clunky non intuitive system not designed for NHS that someone is making a lot of money from. Very disappointed.
“Dad, what was it like before EPIC when you wrote all your notes on a piece of paper?”
50
11
99
What a difference 10 years makes. 10 years ago as FY1 living at Guys Hospital vs. Now

7
0
97
We need. 1. Many more therapists to actually rehab people in hospital.2. Social work working inside health sector, not as separate system.3. A needs first, work out who pays later model to avoid delays about “funding”.4. Much better intermediate care and hospital at home services.
7
11
101
Am now a fully signed up @MRCPUK PACES examiner which is nice but my God we need some more women to examine. If you are a female consultant physician and want more info or check the website or let me know.
18
42
96
“UTI” of the week . Woman seen - TEXTBOOK history of polymyalgia rheumatica. Because of fever, ⬆️ CRP and + urine dip she was seen and discharged with abx for UTI. Represents 5 days later. We gave steroids and 5 days later much improved. Give this geriatrician strength. 💀.
16
8
98
Hospitals are rarely a place where people come in, stay a while, are treated and come out cured. More people are living with increasing complex comorbidity and we have to address expectations early that they probably won’t be the same when they get discharged. #bgsconf.
1
53
92
So my grandad has had a rapidly progressive deterioration over the last 6 months going from no care, to a double handed four times a day package with fast track, now in his last days. They often get such a back rep but I just want to talk about his carers. ⬇️.
14
19
93
I could not agree with this more - and hospitals need to stop referring frail immobile people to an outpatient memory clinic for assessment. Which they physically can’t get to or remember. If it’s really unclear then consider a community memory assessment at home.

geriatricians should diagnose straightforward cases of dementia when everything is clear, even when seeing people as an acute admission. story in @GeriSoc

8
22
100
These discussions are completely easy in 9/10 cases if you approach it right. Everyone makes it so hard for themselves and it just doesnt need to be.
11
7
91
Family friend w met prostate cancer, PSA >150. Pain+weight loss. Oncology: no need to involve palliative care yet, we are not there yet. 🤯🤯🤯. Metastatic cancer or noncurative approach -TELL the patient they won’t be cured and involve pall care early. Please. Good evidence.
7
4
92
On call in AMU last 2 evenings:. 1. Real medicine is back huge breadth of pathology.2. Complexity of patients absolutely sky high need for specialist involvement, much delving into old notes and engaging brain .3. It’s busy again but not with Covid .Great fun.#medicineisbrilliant.
5
3
90
They get paid £9/hr, don’t get paid for travel or between visits. But still they have the thought and care to do this for my Grandma. Why do we treat carers this way? It’s abhorrent. We need to change this. But meanwhile thank you so much, particularly to Linda, Chris and Ali 🙏🏻.
3
10
90
So, it turns out a wide range of views on letting health professionals, esp junior doctors call consultants by their first names. Have had some interesting replies, some raising interesting points. But WTF you lot? Doctors ARE NOT special. ⬇️.
18
7
90
Junior doctors please stop giving patients. ‘STAT’ doses of amlodipine in asymptomatic hypertension ~180. Just not needed. Reassure and educate nursing colleagues who are concerned about why. Also remember mirabegron which you will see more often can cause. hypertension.
20
38
81