

Me
@mattdoc1988
Followers
1,314
Following
2,885
Media
749
Statuses
6,973
Intensive Care Medicine & Anaesthesia Consultant. Married to cycling, running, holidays & wife (any order). @thepoppystudy coinvestigator
Devon, South West, England
Joined December 2015
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Elon Musk
• 471407 Tweets
Champions
• 378502 Tweets
Alexandre de Moraes
• 361952 Tweets
Brazil
• 349956 Tweets
Se o Twitter
• 317584 Tweets
Colorado
• 264759 Tweets
Mbappe
• 224452 Tweets
لاس بالماس
• 195862 Tweets
Real Madrid
• 184778 Tweets
Beşiktaş
• 177815 Tweets
Xandão
• 102218 Tweets
Bluesky
• 77522 Tweets
Hermoso
• 70874 Tweets
McDonald
• 67159 Tweets
Kutlu Olsun
• 67072 Tweets
Mustafa Kemal Atatürk
• 59866 Tweets
#BJKvLUG
• 54141 Tweets
#الاتحاد_التعاون
• 53963 Tweets
كاراسكو
• 47524 Tweets
Vini
• 38466 Tweets
#30AgustosZaferBayramı
• 35944 Tweets
LIBERTÁ IS OUT
• 32761 Tweets
Amrabat
• 29534 Tweets
Rafa Silva
• 29418 Tweets
Brahim
• 21896 Tweets
Servette
• 21512 Tweets
避難指示
• 20933 Tweets
Ancelotti
• 20930 Tweets
Tchouameni
• 19020 Tweets
#خلصوا_باكايوكو_للهلال
• 18900 Tweets
緊急速報
• 17771 Tweets
Modric
• 16681 Tweets
Kroos
• 16246 Tweets
Abdullah Avcı
• 12575 Tweets
Jack White
• 12007 Tweets
多摩川氾濫
• 11580 Tweets
Valverde
• 10868 Tweets
Mendy
• 10128 Tweets




















The reality of Intensive Care at the moment…
A Covid patient admitted to ICU means another patient cannot have their brain tumour operated on or their stomach cancer removed.
It’s one patient in, one patient out.
Some Covid admissions are avoidable.
#GetVaccinated
21
437
2K
A thread about ICU admission decisions
There seems to be lots of (mis)information about how intensive care doctors decide whether a patient would benefit from coming to ICU. I thought I’d try and explain some of these decisions - relevant to Covid and more generally.
1/n

30
505
842
Start a new job this week. 🤓
1 hour commute. 😴
Told there’s no parking available on site during the day. 😱
Hospital suggest I use park & ride - adds another 20 mins onto my drive. 🤬
Welcome to medical training. 😐
77
61
773
Cardiac arrest on surgical patient.
Me: “This patient has been in a non-shockable rhythm for 30 minutes. Does anyone think we may have forgotten anything?”
Surgeon: “Can you make them go into a shockable rhythm somehow?”
19
16
303
@LozzaFox
Pertussis is whooping cough, a bacterial lung infection. The reason you haven’t heard of it is because we are vaccinated against it in childhood. Therefore, you are not aware of people suffering from pertussis. Which is the whole point of vaccines.
8
2
199
‘Interesting’ case.
Dementia, significant sacral sore, NH resident.
Resources used:
CT head
CT abdo/pelvis
MRI head
Abdo USS
EEG
ICU stay with I&V
Apart from anything else, where is the dignity in dying & pragmatism in end of life care?

It’s a great case with a positive outcome and some learning points.
But, 70, in a NH, multimorbid….
I worry about duration of delirium, persistence of lung injury and deconditioning.
It shows the discrepancy between NHS and US (?comprehensively insured) healthcare.
15
5
87
17
7
154
In conclusion, when admitting someone to ICU, intensivists consider:
- The current illness
- The baseline function of patient including other illnesses
- The patient’s wishes
18/n
8
18
134
To add to the argument of ABG vs VBG...
Why don’t we use capillary blood gases (CBG) more often in adults?
Seems to give a pretty accurate result in kids.
Never seen it used in adults. Same effort as measuring blood glucose.
42
8
130
@berger_nicky
@HorsleyCarl
Unfortunately life doesn’t work like that. That would mean no one should ever make a mistake. Systems, especially in healthcare, are complex. Many opportunities of errors to occur. We try to reduce these but it’ll never be completely error free unfortunately.
3
1
123
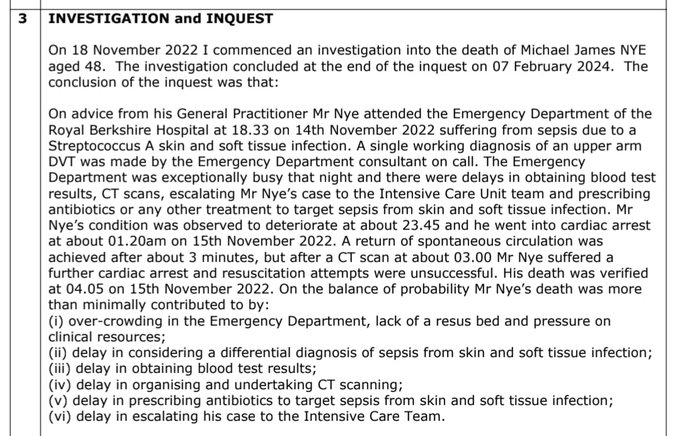
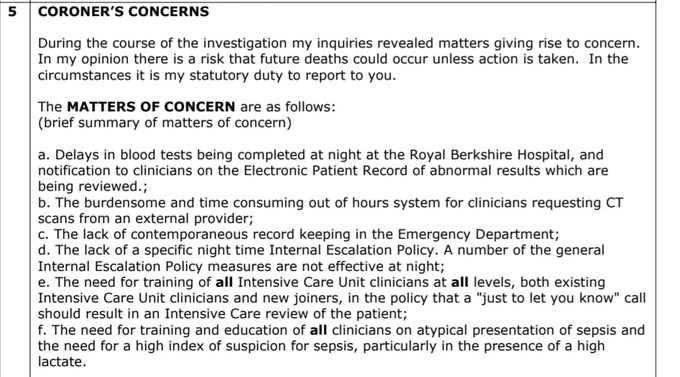
Coroner’s report stating all ICU referrals saying “just to let you know” should result in an in person review of the patient.


🚨 The
@RBNHSFT
A&E seems risky out of hours! Coroner says overcrowding in A&E was one factor that contributed to a man's death...
28
103
232
31
21
113
@nikosevangelou3
Sorry to get nerdy but it’s actually nitrous oxide (N2O).
Not nitric oxide (NO).
🤓
4
3
111

To all doctor colleagues. I think we should all back
@Jeremy_Hunt
as Tory leader. He's supported us so much recently I thought it'd be nice.
4
58
80
When the surgical SHO explains the concept of ‘permissive hypotension’ to me in a bleeding patient & advises I should aim for a BP of 50 systolic. Well she’s unconscious so maybe we should perfuse something?
7
3
77
How do we move away from this idea that patients HAVE to have surgery before they die?
Statements like this really irritate me...
“If you have surgery your mortality is 40%, but if you don’t have surgery, it’ll be 100%.”
21
8
78
Moet in the fridge for this evening.
Passed
#FFICM
MCQ 🥳
Now just need to think about this viva/OSCE. Any tips?
#theendofexamsisinsight
#moetmedic
3
0
73
Recent oncall felt like a proper RCOA/FICM viva:
-Anaesthetised 2 year old for supracondylar fracture
-Transferred head injured patient to neurosurg centre
-Cardiac tamponade to the cath lab for pericardiocentesis
-Ethylene glycol poisoning.
Exhausting, but I do love my job! 😁
1
0
73
@aroradrn
My wife’s grandmother (from Thailand) reheats cooked rice on the wall in the sun in the back yard. 😮
She’s doing very well still!
1
0
67
If they are very weak, frail and deconditioned, they are less likely to have the ability to fight the disease. This is what we call physiological reserve - how good is their body going to be at fighting this disease?
7/n

5
14
61
I’ve been fast bleeped to NICU for airway difficulties on a few occasions as anaesthetic SpR. Also managing collapsed neonate in ED.
NICU have v different approach to airway management - I have never come across in any other clinical practice (inc adult & paeds anaesth & ICM)

@thatsnotmine125
@VirtueOfNothing
@telswood
@Matt_L_Nash
This does seem a bizarre conversation
Intubation of the critically ill adult is rife with risk & complications. Harm is common.
Intubation of the neonate (especially when critically ill) is a league up in failure, delay & complications. Harm is intrinsically less easy to
12
51
311
9
5
61
Actual age is irrelevant. It is physiological age that matters. If they are an 70 year old with no medical problems and active they have a much better ‘physiological reserve’ than someone in their 50s who has had multiple heart attacks, ...
8/n

1
15
60
@SteveBarclay
@BMA_JuniorDocs
Your door is as open? Well then just start talking to the BMA then rather than playing politics.
0
2
60
@JonBall
If you pave that close around a tree that size then you’re going to kill the roots. Fairly predictable. Who designs pavements like that?!
2
1
51
Recovery beyond ICU is essential. Leaving ICU is just the start of a journey with critical illness. Many people take months-years to recover from an ICU illness.
11/n

1
8
52
A challenging case that highlights the risks of giving sedation in an acutely unwell patient with obesity in difficult circumstances.
A 38-year-old black man died at
@NHSBartsHealth
after a flawed decision to sedate him. Coroner criticises "coping culture" and the trust response including governance failures and poor effort by lawyers
#patientsafety


51
170
373
8
3
53
been in and out of hospital with difficult diabetes, has bad kidney function and can’t manage to walk more than 50m before getting short of breath.
Our machines and drugs can support the body, but ultimately the patient has to be able to support themselves.
9/n
2
5
45
Serious illness leads to loss of muscle tissues, weakened immune systems, worse brain function (confusion, memory loss, PTSD), poor cough, shortness of breath, to name a few problems. People have be able to be strong enough for rehab and get through this recovery phase.
12/n
1
9
43
@Iromg
@LoftheBridge1
You can’t train to be a consultant in private hospitals. So juniors doctors don’t work in private hospitals. We have to work for the NHS.
3
1
45
Perhaps, worse would be if they got through their admission, but then died on the wards later on because they were too weak to recover from their illness. The traumatic experiences & struggles of getting through an ICU stay need to be worth it - for the pt, their family
16/n
1
5
43
ICU isn’t a magic treatment. We offer organ support, e.g. ventilation, or blood pressure support, to help the sickest patients recover from their illness. It offers high levels of nursing & medical input and close monitoring.
2/n

1
6
43
It is not a treatment in itself and the patient has to be able to get better - ICU supports them do this.
There a key considerations intensivists will make when considering if someone should be admitted to ICU...
3/n
1
4
42
@when_cats_away
@LeeHurstComic
Thanks. Even in the middle of a pandemic people can’t be nice to others. NHS staff really appreciate your feedback. 🙄
1
0
44
Patient’s wishes:
We alway ask patients how they would like to be treated. We won’t offer treatments we think are futile - will have no difference to their outcomes.
13/n
3
5
40
If patients are too unwell to tell us, then we ask family. This is not to ask what the family would want to happen to their relative. It is to gauge whether their ill relative had previously said what they would like to happen to them if they were be become very unwell.
14/n
1
4
40
Do they hate being ill and going to doctors? “They’d never want to end up on a ventilator and stuck in a chair all day” is a common thing relatives tell us. The last thing we want to do is put someone through an ICU admission if they never want it.
15/n
2
5
38
These are complex & difficult decisions. Different Intensivists may make different decisions. There are no right answers. A collective approach of with intensivists, specialist docs with patients & their families, we hope we make the right decision for each patient.
17/n
1
4
37
Covid is a good example where, for some patients, they do not need to come to ICU as they may be fine on facemask oxygen or NIV facemask on the wards. Some may need to come in a few days perhaps.
5/n

1
4
34
Recoverability
If the acute illness is so bad, then whatever we do, ICU will not change the outcome. The illness maybe recoverable in a fit person, but perhaps the patient has so many other medical problems their body won’t be able to cope with the illness ontop.
10/n
1
5
35
I don’t quite understand this.
Surely a vaccine can be delivered by a ‘technician’. Why does a medical professional need to be do this?
GP would be much better placed doing medical things?
5
4
36
@jon1467
A 4th year med student, having spent a day in theatre, once asked a consultant anaesthetist “What do anaesthetists actually do?”
8
0
35

The current illness:
What is the patient ill with? If it is a pneumonia, how serious is it? How much oxygen are they requiring? Is their breathing laboured? If their pneumonia is very bad and they maybe need ventilation, is this going to help the patient get better?
4/n

1
3
29
Multi source feedback should just ask one question… “This doctor is a good egg?” Followed by space for free text.
Having to fill an MSF for an ED trainee recently… about 30 questions, many requiring free text for individual attributes.
Why make it so complicated?
5
2
33
Maybe I’ve seen too many sick Covid patients in hospital recently…
As I walk around the supermarket and see so many people not wearing masks, I imagine them all sitting on the Covid ward or on ICU.
😷
Can help but fear a terrible winter!
4
2
33
Their longterm illnesses and physical state
What can this person do normally? Are they able to run a marathon? Or are they bed bound? Are they are physically fit normally or conversely frail? If so, they are much more likely to be able to fight the disease and recover.
6/n
1
4
29
@SteveBarclay
You make it sound like you’re giving it to them willingly. They did go on strike to get that from you!
0
1
31
@tombircher
Or they could be cared for in special beds inside rooms, looked after by doctors and nurses called…
Helping Old & Sick Patients Inorder To Alliviate iLlnesses
Just a thought. Especially, given winter pressures. 🤷♂️
1
0
31
Amazing support from Consultants at Royal Devon & Exeter Hospital for
#juniordoctors
.
@TheBMA
@johannmalawana

0
29
27
@DGlaucomflecken
@DrEricStrong
@CaseMcQuade
I’m pretty sure the stroke doctors do something about strokes occasionally.
1
0
30
@DrRJWebb
It definitely exists. Grossly oedematous but any hint of diuresis they become hypotensive and/or hypernatraemic.
My approach is…
1 do they need diuresis. Can they do it themselves?
2 go gentle - low dose with a combination of diuretics (furosemide, spironolactone, metolazone)
2
0
29
@PictonChris
@RoyalAdelHosp
@SteveBarclay
@RishiSunak
- sponsoring the Australian health system.
#NHS
@NadineDorries
- maybe think about what other systems are doing right/better before trapping doctors in NHS.
0
2
27
Copy of
@BJAJournals
arrived in post today. Couldn’t help noticing, whilst the Anaesthetist & ODP are calmly inserting a cannula, the patient’s oxygen sats appear to be 79%. Arm doesn’t look hypoxic though I guess.

8
0
29
@David_Cameron
@Jeremy_Hunt
Seems like ur example of uniform 7 day elective work at
@SalfordRoyalNHS
isn't true.


4
65
27
Would b great if the NICU and PICU/Anaesthesia could share airway learning together. Airway practice on PICU is v closely aligned with Anaesthesia (Paed & adult) & adult ICM practice. Neonatal airway practice seems to be different. I’m sure we have a lot to learn from each other
1
0
27
@EmergMedDr
@CdoggMiller
@VictoriaLIVE
So he’s done F1/2. How does that make him a ‘junior surgical doctor’? That means I’m a junior surgical doctor too! Snap! He probably did one surgical job once during F1. What’s more important is if he’s done Obs & Gynae really. They’re the ones that do abortions, not surgeons.
1
2
25
@PBSherren
Always seems to be the people that are most vulnerable to Covid, and most likely to get severe Covid, that would benefit the most for wearing a face mask but are ‘exempt’… 🤷♂️
“My severe asthma stops me wearing a face mask”.
2
0
27
@Resuspiece
In addition, my real bugbear (initially) of not giving contrast for CTs in unwell patients because of ‘the kidneys’.
1
0
27
One thing I have learnt on Paediatric ICU so far...
Proning a kid is much simpler than in adults.
2
0
27
Colleague said that when he takes ICU referral he doesn’t ask questions & heads straight to the patient. Says it “gives people a hard time” if you ask more details.
Couldn’t agree less. How do I know how to prioritise my work if I just drop everything & come running?
17
2
27
These comments are not helpful. You can’t quote 97% mortality in ventilated Covid pts and then paste the reference as a range 81-97%. And completely ignore the early UK
@ICNARC
data. All data sets are small. Also, UK ICU admission criteria often v different.
Scares the public.

Why is everyone so caught up in the ventilator love myth?
If you get put on mechanical ventilation, you have about a 97.8% chance of dying.
Yes we need lots of ventilators.
No, they will not prevent the vast majority from dying.
#Covid_19
38
53
270
2
1
26
I find it odd as an ICM trainee I have had no further training in breaking bad news or difficult conversations since I left med school.

Today I watched 10 doctors try to have a DNACPR discussion in the context of discussing a deteriorating patient.
Even those most skilled in communication made the task so much more difficult that it needed to be.
@DrLindaDykes
we need to sort this out
⬇️
42
147
460
9
4
26
@IM_Crit_
But would you let a patient choose a chemotherapy that had no benefit for their cancer?
Or an antibiotic that we knew their infection was resistant to?
Why is CPR different?
3
2
25
@IM_Crit_
200 beds would be a pretty small hospital in the UK!
All ICUs staffed by intensivists but some smaller ones share oncall rota with anaesthesia.
I guess the geography of UK is very different to the US.
3
0
24

@WelshGasDoc
Oh no, I’m about to be very ill.... I need to drive somewhere! 🧐
Maybe need to look at
@DVLAgovuk
regulations?
0
1
22
If only there was a 5-6 year lead in time for the UKFPO to prepare for the graduation of these med students….
🤔

Glad this has been finally picked up but some important qs remain: are incentive payments being used to create new jobs quickly & what is being done to avoid a larger mess next year?
14
56
149
0
3
24
SHO doctor rota gaps in Emergency Dept in hosp near me
#mindtherotagap
@Jeremy_Hunt
@HackneyAbbott
@sarahwollaston

7
57
22
@_skylined_
Kate. I’m so sorry you are going through this. (Slightly depends on individual hospitals) but there is often support for post-ICU patients. Follow up clinics where you can seek help with understanding what you’ve gone through. They can link into psychological support.
0
0
23
@Jeremy_Hunt
I've already sent u 2 invites to shadow me at work. Still haven't heard back. I'm getting quite upset now Jeremy. Please RSVP.
2
16
21
Having an NSAID around the time of endurance exercise could be dangerous.
Voltarol is sponsoring the London Marathon!
Someone think of the kidneys!!!

Voltarol is the new Official Pain Relief Partner of the TCS London Marathon.
This innovative partnership will cover the 2024 and 2025 events and involve:
✅ helping participants prepare for the event by providing guidance on tackling pain
✅ providing entertainment at Rainbow

9
6
37
2
2
21
This is really great idea for
@wesstreeting
A central library of NHS guidelines (both local and national).
Why have 1000s of separate guidelines for each hospital across the UK when we could share many (or at least make minor local amendments).
3
2
18
@Med_Registrar
Don’t think I’ve ever asked the medics to attend in person. But needs to be really clear what samples need sending and how.
0
0
19
@drokane
This is quite old school. However, I think it’s important a consultant/senior doc should be involved in the original referral & then needs to be discussed with ICU consultant regardless. The more complex the patient there definitely should be consultant to consultant discussions
3
0
20
@doctorrxg
@ICU_Management
We do offer ‘treatment’ - antibiotics, draining infections, anti-epileptics, etc.
But ECMO, ventilation strategies are not treatments. They temporise things. They don’t effect the underlying disease. They prevent lung injury and allow time for recovery & allow Abx to work.
2
2
19
@Microbedoc2
I do think switchboards should have a statement for each specialty overnight.
“This specialty has a 24hr on call. Are you sure you want me to put you through?”
Or non-resident oncalls should be slightly protected between say 2am-6am with switch checking it’s a true emergency.
2
2
20
@iainpdooley
@fhussain73
@NHSEngland
@rankinphoto
The vaccine is not compulsory. No one is making anyone have the vaccine against their will. However, there is a lot of misinformation out there and some apathy so a gentle nudge from your trusted GP may change a few people’s minds. Excellent work
@fhussain73
2
0
18
@johnestevens
Sounds a very sensible idea. As long as people satisfy the set criteria they can have it. It’s technically very easy to administer.
0
0
18
If NICU trainee&cons struggle with intubation exposure with limited case numbers in DGH, perhaps tertiary centres should (maybe they are?) offer refresher opportunities to keep skills up to date? There clearly are the numbers if their cons&ANPs are intubating 1000s of babies?
1
0
19
What is this LMA... ?
3 months Cardiothoracic and 2 months Neuroanaesthesia.
1st plastics list in months!
1
0
19
@ncl_medic
@guardian
This is why it’s not called brainstem death! Should be called ‘death by neurological criteria’.
It’s a confusing concept for medics/lawyers… let alone grieving parents! So we should keep it as simple as possible: “he has died”.
1
0
18
@cindylou12
@ReevePara
@Danielf90
Usually on ICU we put them in the ‘superman’ position with one arm in front crawl position and head to one side on a pillow.
There are many proning contractions we normally use in theatre for e.g. spinal surgery but not usually appropriate for ICU.
0
2
18
I get the feeling
@NHSE_WTE
must have said a few years ago that specific courses (inc ALS/ATLS etc) should no longer be compulsory on training curriculum - to save them £££ in their study budgets.
🧵

This is becoming an absolute joke in the UK. We are devaluing education and training.
These are VERY BASIC life support courses that are the alphabet of in-hospital resuscitation.
Every doctor needs to have done it. Not on their own dime as an optional extra.
6
31
183
1
1
18
On NICU I asked for airway trolley & difficult airway algorithm/checklist- the SpR returned 20min later with 20page guideline they’d printed off BAPM website
Given 5 doses of sux back to back
No videolaryngoscope
Always turning down the O2 even when sats 70%
No LMA available
2
0
18
Everything that is wrong with medicine - the system is set up to act contrary to the best interests of the patient.
Some of the most rewarding & meaningful times in medicine are doing less: not giving a medication, not performing an operation, not admitting to ICU….
1/2

Dad spent two of the last days of his life alone and distressed in A&E – for no good reason. This insanity must stop | Adrian Chiles
28
70
210
2
3
18
Please please please just stop spouting lies and concentrate on sorting out this mess. Stop spinning. Infuriating.

.
@Jeremy_Hunt
: the resumption of talks shows the Govt’s door is & has always been open to meaningful talks
#HealthQuestions
#JuniorContract
135
4
1
0
18
15
@DrHoenderkamp
@DocAnonX
@DianaBlackburne
@drdavidbull
@prema14
Renee, if you could detail the tuition fees you paid when you went to medical school?
Students now pay £9000/year to study medicine. It’s not free or paid for by government. It’s subsidised but certainly not free.
1
0
17
@Jdon101_
When I did an ED job, I wished something existed for ED docs similar reasons. Would be SO educational to get that feedback. We had access to discharge summaries so I would save some hospital numbers & look them up on a quiet shift.
0
0
18
@JackBarton07
Functional/social history really important. No one ever documents it again after admission but it’s key for ICU reviews. Gives an idea of physiological reserve. Keep it simple - can they climb flight of stairs, walking distance, do own shopping/ADL, occupation, driver… ?
2
0
17
@TurtonsOther
@MedCrisis
I had an ICU sister once tell me to “leave the unit and go to bed” because there was nothing to do! 🤩
0
0
17
Best analogy I’ve heard regarding enforcing face mask wearing in hospital now we’re past the peak...
“It’s like wearing a condom to the 12 week pregnancy scan”
1
2
17
@rupert_pearse
Do you have data on ICU & hospital admissions and the patients’ vaccine status? Can’t seem to find this info easily?
3
0
17
Got introduced to a patient, by a pre-op nurse, as the “little man who assists the anaesthetist”.
What would you say to the nurse in response to this?
Ignore it 🤐
101
Say it was patronising 🧐
211
Say you’re Anaesthetist 🤓
272
Have a fit of rage! 🤬
61
28
1
17