
Neudrawlogy
@neudrawlogy
Followers
8,138
Following
247
Media
50
Statuses
294
🎨 Infographics and tweetorials in Neurology 🧠 • ➡️ ⬅️ • Posts are for educational purposes only • Founder @gabifpucci
#NeuroTwitter
Joined July 2021
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
CHEER UP ARTIST FOURTH
• 93786 Tweets
#PKAtelier24xZNN
• 46703 Tweets
#ヒロアカ
• 37250 Tweets
PKAW 2024 x NuNew
• 31376 Tweets
花火大会
• 18676 Tweets
オースティン
• 15037 Tweets
ファーム日本一
• 12485 Tweets
WALK WITH ENHYPEN IN GOYANG
• 11653 Tweets
Badminton With Patrick
• 10170 Tweets



















Introducing
#NeudrawlogyCR
for our
#ClinicalReasoning
infographics!
The first one: approach to Chronic Daily Headache! 🤕🧠
Click the image to view the entire infographic, or see it on the website
Special thanks to Dr. Robert Kaniecki for reviewing it!

1
209
710
Hello,
#NeuroTwitter
!
Are you ready to learn about hemineglect? 🧠🎨
Thank you
@tirthasawant10
for collaborating to create this new infographic!
#FOAMed
#MedEd
#Neurology
#EndNeurophobia
Check the website to see all the infographics ➡️

4
98
439
Happy Friday,
#NeuroTwitter
!
🧠Delve into the anatomy & clinical ties of the Internal Carotid Artery with this must-see infographic! In collaboration with
@LucasRochaMD
Kudos to
@SitaraKoneru
&
@Nirav_r_bhatt
for the inspiration & review!
#EndNeurophobia
#Neuroanatomy

5
108
366
🧠Have you ever had to perform a
#LumbarPuncture
?
Check this infographic, and perform your champagne tap* 🍾🥂💉!
#MedEd
#FOAMed
#NeuroTwitterNetwork
#NeuroTwitter
*lumbar puncture with no cerebrospinal fluid red blood cells 🚫🩸🧪

3
110
353
Welcome to the
#NeudrawlogyMigraineEdition
! 🤕 🧠
This first
#infographic
contains the diagnostic criteria for Migraine Without Aura, and in this series, you will see other essential features of this prevalent disease.
🧵 1/10
#Tweetorial
#NeuroTwitterNetwork
#FOAMed
🧠📚🎨

8
120
343
#NeudrawlogyMigraineEdition
, part 5! 🤕 🧠
Here goes a review of the preventive treatments for migraine! 🧵 (1/10)
✅ Learn here:
🎯 Indications;
💊 General recommendations about the treatment.
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd
#MedTweetorial

5
97
324
Neurologic 🧠 manifestations of Tuberculosis 🦠 in one image!! 🤩
#NeuroTwitter
#Neurotuberculosis
#MedEd

0
85
320
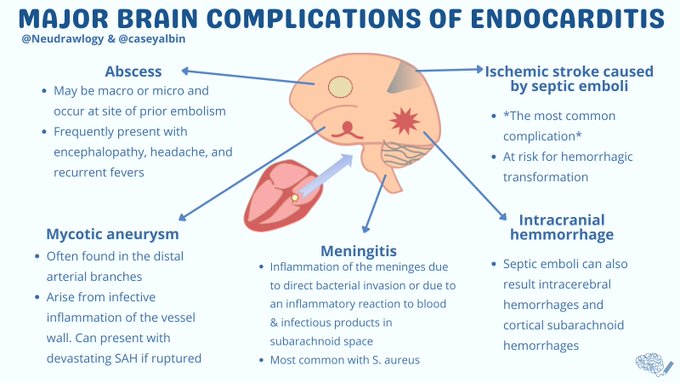
1/
It was a delight to work with
@caseyalbin
to explore the incredibly diverse CNS complications of infective endocarditis!
An
#infographic
&
#tweetorial
investigating the radiographic & clinical findings in IE, with some management pearls.
#MedEd
#Neurotwitter
3
92
304
Hey,
#NeuroTwitter
, are you feeling down? 😢
Check the new infographic about CN 3 palsy!
The clinical manifestation of a complete ophthalmoplegia is known as "Down and Out Syndrome" due to the eye position! 👁️👁️
🧠📚🎨

1
80
284
#ItsAllAboutPupils
episode 4!
Johann Friedrich Horner was a Swiss🇨🇭ophthalmologist. In 1873, one of his students published a thesis describing a woman with "oculosympathetic paresis".
A short🧵containing history and a bit of scientific gossip! 🙊
🧠📚🎨

2
77
242
#NeudrawlogyMigraineEdition
, part 4! 🤕🧠
⏰A migraine attack lasts up to 72h, and can be disabling.
Here goes a review of the pharmacologic 💊 and nonpharmacologic 🏞 treatment of an acute migraine attack🧵! (1/16)
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd

4
78
234
#NeudrawlogyMigraineEdition
, part 3! 🤕🧠
Migraine is an inherited disorder 🧬of sensory processing with 5 defined phases.
They do not need to occur in every person or even in every attack, and they may overlap.
A 🧵! (1/5)
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd

4
69
235
A diagnosis that you can't miss: Wallenberg's Syndrome 🔥
- A
#DDx
for Acute Vestibular Syndrome 😵💫!
(Not shown in the infographic: hiccups ➡️ associated with reticular formation lesion)
#NeuroTwitter
#MedEd
#FOAMed
🧠🎨📚

2
65
226
Tolosa-Hunt syndrome is a rare disease that presents with headache 🤯 and diplopia 👀👀!
Check the infographic to learn more🧐
#NeuroTwitter
#MedEd
#FOAMed
🧠📚🎨
(1/4)

3
65
227
🧮Just do the math: 1 + 2 + 3 + 4 = Gerstmann Syndrome!
#NeuroTwitter
#NeuroTwitterNetwork
#MedEd
#FOAMed
📜Historical fact: it was first described in 1924, by Josef Gerstmann, and Austrian 🇦🇹 Neurologist, after evaluating a patient with a stroke!
🧠📚🎨

4
57
211
Excited to announce that we are now a WEBSITE too!!
🧠🎨💞
We are so thankful for our followers and friends from the
#NeuroTwitterNetwork
community!
#NeurologyProud
#AANAM

3
47
188
Sorry for bringing you step 1 📝 memories...
Thiamin is a cofactor for several key enzymes responsible for the maintenance of cerebral energy homeostasis ⚖️ !
An acute thiamine deficiency can cause Wernicke Encephalopathy 🧠⚡️!
🧠📚🎨

2
58
180
🎉Almost 1,5k fantastic neuro nerds follow this page!
So here goes an infographic about
#OneAndAHalfSyndrome
!
One eye doesn’t move horizontally, and the other can only abduct! 👀
PS: For me, it makes more sense to think of it as “Zero-and-a-half” syndrome ... 😂

2
42
179
🍭Are you ready to go back to your childhood,
#NeuroTwitter
?
Because ... today's topic is Alice in Wonderland 👧🐇🎩!
(Isn't neurology the best specialty ever?)
Thanks to our Instagram followers who chose this great topic for today!
🧠📚🎨
#FOAMed
#MedEd

5
44
173
Follow-up of Wernicke Encephalopathy: here goes Korsakoff Syndrome!
Confabulation 💭 + anterograde amnesia 🧠!
#MedEd
#NeuroTwitterNetwork
#FOAMed
🧠📚🎨

1
36
168
Dear
#NeuroTwitterNetwork
,
We are proud to share a review of the CNS manifestations of SLE 🧠 !
🔥 A collaboration with
@MithuRheum
from
@RheumOnePagers
!
#LupusAwarenessMonth

1
40
160
Welcome to the
#NeudrawlogyMigraineEdition
, part 2! 🤕🧠
Aura is a Greek 🇬🇷 word and deity that means breeze 🌬, and in medicine, it is a symptom that occurs in up to 25% of people with migraine.
A 🧵! 1/7
#NeuroTwitter
#NeuroTwitterNetwork
#FOAMed
#MedEd
#MedTwitter
🧠📚🎨

2
43
150
Douglas Argyll Robertson was a Scottish 🏴 ophthalmologist 👁️who described this pupil in 1869 in a patient with neurosyphilis 🦠.
He also first described the effects of physostigmine, extracted from Calabar bean 🌿, which he tested on his own eyes!
#NeuroTwitter
#FOAMed

1
44
149
#ItsAllAboutPupils
!
Another famous pupil 👁️ is being featured!
📜Robert Marcus Gunn was a Scottish physician, that in 1902 described the "pathologic pupillary escape". Later (1959), Levitan better characterized this finding with the swinging light test 🔦.
Thoughts?
🧠📚🎨

3
45
148
The sun has almost set 🌇, which reminded me to post another infographic!
👀The impaired up gaze of Parinaud's Syndrome can lead to a preference of looking downwards, which resembles a sunset 🌞
#NeuroTwitter
#MedEd
#FOAMed

3
39
139
Another incredible collaboration with the one and only
@caseyalbin
!
Learning the important aspects of the coma exam is key, so come and take a look at the this new infographic!
#NeuroClerkshipTips
#NeuroTwitter
#NeuroX
#NeurotwitterNetwork
#FOAMed
#MedEd

3
46
141
Pseudobulbar affect can be very distressful... have you ever heard of this manifestation?
Thoughts,
#NeuroTwitter
?
#NeuroTwitterNetwork
#MedEd

4
33
117
#NeudrawlogyMigraineEdition
, part 6! 🤕🧠
Did you know that migraine has different presentations in children 🍭 compared to adults? 🧵 (1/12)
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd
#MedTweetorial

4
31
117
#CerebellumIsNotGuilty
Check this new schema about the Romberg's Test, and stop blaming the cerebellum!
🧠📚🎨
Thoughts?
#NeuroTwitter
#NeuroTwitterNetwork
#MedEd

1
26
104
Since yesterday's post was Korsakoff Syndrome ... We decided to dive into confabulation 🧠🌈 today !
🤓🤓
Infographic made in collaboration with
@FTeixeiraMD
!
Thoughts,
#NeuroTwitter
?
🧠📚🎨
#FOAMed
#MedEd
#NeuroTwitterNetwork

0
18
92
Welcome to
#NeudrawlogyMigraineEdition
, part 7! 🤕🧠
CRGP = Calcitonin gene-related peptide plays an important role on the pathophysiology of migraine
💊Their antagonists can be used for either migraine prophylaxis or acute treatment of a headache episode
Part 8 tomorrow!

2
16
86
#NeudrawlogyMigraineEdition
, part 8! 🤕🧠
Today, we continue our review on CGRP antagonists for migraine!
See here the doses, indications and side effects.
#NeuroTwitter
#MedEd
#FOAMed
#NeuroTwitterNetwork

1
22
69
#ItsAllAboutPupils
!
William Adie was an 🇦🇺 neurologist who bravely worked in World War 1 💣 with traumatic brain injury.
He and his friend Gordon Holmes independently described this finding in 1931!
What else is he famous for? Can you guess? 🧐
🧠📚🎨
#NeuroTwitter
#FOAMed

1
16
71
Happy to be featured on the
#HowToNeuroTwitter
2.0 Guide!
Thank you
@aszelikovich
and all the amazing people from
#NeuroTwittterNetwork
🧠💜
Check the full guide below ⬇️


#NeuroTwitterNetwork
#HowToNeuroTwitter
2.0 Guide is LIVE! 👉
-This (FREE) guide created by 🧠's for 🧠's at ALL stages of training, especially to M4s applying
#neurology
@NMatch2022
-Please RT, Share, & Use the guide w fellow neurologists on Twitter!
3
98
191
0
9
62
If you love 🧠 and 🎨, here's a special infographic for you!
💡How can neurological disorders change the creative process?
Let us know what else you have,
#NeuroTwitter
!
*Created in collaboration with
@MariaMjaleman
- check her fantastic tweetorial below!


Do you think creativity can be pathological? 🤔
Neuro says: maybe🧠❤️
What differential diagnosis can you come up for the CC: "new or improved bursts of creativity"? ⚡🔥
(Sorry for the made up schema, don't quote me on this)
#art
#neurotwitter

6
21
89
2
20
61
Did you miss something? 👀🙈
See below all the infographics that I posted so far ⬇️😍
#NeuroTwitter
#NeuroTwitterNetwork
#MedTwitter
#FOAMed
#EndNeurophobia

2
14
46
Such an honor to work with the one and only
@MarcusVPinto
on this infographic about Amyloid neuropathies!
Check our infographic here, and make sure you read the excellent tweetorial from
@PNSociety1
below!
#NeuroTwitter
#EndNeurophobia
@Grepmed
@MedTweetorials


2
8
41
11/
Similarly, meningitis is another infectious complication. Most commonly with S. Aureus!
The 🔑: whatever abx are being used for the endocarditis MUST have CNS penetration (no cefazolin!)
A table of abx with good CNS penetration
@meganRx1
from
#AcuteNeurologySurvivalGuide
.

2
5
26
#ItsAllAboutPupils
- a must read
#tweetorial
by
@AaronLBerkowitz
Also, see below the previous infographics involving pupils 👁️!
🧠📚🎨
#NeuroTwitter
#MedEd
#FOAMed

It’s time for another
#EndNeurophobia
#tweetorial
!
PUPILS AND ANISOCORIA
#MedStudentTwitter
#neurotwitter
#MedEd
@DxRxEdu
@rabihmgeha
@CPSolvers
@Tracey1milligan
@NMatch2022
🧠❤️
8
112
361
1
6
20
Read the original article about this rule here:

1
2
18
1/ Migraine’s pathophysiology is very complex and involves:
- Primary neuronal dysfunction
- Cortical spreading depression of Leão (it is thought to cause both the aura and the headache)
- Activation of trigeminal afferents causing inflammation
1
1
16
6/ There are four groups of Primary Headache Disorders: 1) migraine, 2) tension-type headache, 3trigeminal autonomic cephalalgias, and 4)other primary headache disorders.
1
1
15
13/ Thoughts and additions??
@AaronLBerkowitz
@rabihmgeha
@DxRxEdu
@MattiaRosso3
@Marinos_S
@Dr_Ighodaro
@MarcusVPinto
@mendesthiagob
@IsaMathiasMD
@CardioNerds
@rav7ks
@grepmeded
@RosenelliEM
@GabrielBragaMD

5
0
15
Tune in tomorrow to see the new website that will be launched with all our
#infographics
!
We will see you then!
@AANmember
#NeurologyProud

I am super excited to present my work on
@neudrawlogy
tomorrow at
#AANAM
!
Thanks
@caseyalbin
for your help and all the
#NeuroTwitter
family for this amazing community!
#NeuroTwitterNetwork
@AANmember
#NeurologyProud
@upmcneuro

7
8
73
0
1
15
🧐References 1/2:
Kimberly S Johnson, MDDaniel J Sexton, MD. Lumbar puncture: Technique, indications, contraindications, and complications in adults In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on October 24, 2021.)
1
2
14

If you want to know more about a pathology affecting the cavernous sinus - TOLOSA HUNT SYNDROME:
OR
Tolosa-Hunt syndrome is a rare disease that presents with headache 🤯 and diplopia 👀👀!
Check the infographic to learn more🧐
#NeuroTwitter
#MedEd
#FOAMed
🧠📚🎨
(1/4)
3
65
227
1
0
13
4/ … And migraine alone is the third disability cause among people aged 15-49 years old. It is more common in women.
1
0
13
Original tweet here:
The answer is Parinaud's Syndrome! Here's a schema that I did.
Thoughts,
#NeuroTwitter
and
#MedTwitter
?
#MedED
#EndNeurophobia
#FimDaNeurofobia

5
24
78
0
2
13
0
2
13
3/ But… each person is different, and, again, migraine is a complex disease. Many other triggers are not listed above and not yet studied, so a careful history and a headache diary are essential steps in the treatment!
1
1
12
5/ Here are some the general recommendations 💊
Some authors suggest initial treatment with any of these 4 drugs since they work in 50% of the patients:
- Amitriptyline
- Propranolol or metoprolol
- Topiramate
- Venlafaxine
1
1
11
5/ Approaching a patient with a headache:
Is it primary or secondary?
A correct diagnosis is imperative for adequate treatment.
1
0
11
3/ Headaches are the second leading cause of years lived with disability worldwide…
1
0
11
... because the first eye does ZERO movement and the second eye does only HALF of them 😂
But PLEASE let's keep the correct name! ✅
2
0
11
6/ Parinaud's Syndrome ⬇️
The sun has almost set 🌇, which reminded me to post another infographic!
👀The impaired up gaze of Parinaud's Syndrome can lead to a preference of looking downwards, which resembles a sunset 🌞
#NeuroTwitter
#MedEd
#FOAMed
3
39
139
1
3
11
If you want to localize the lesion using the Rule of Four of the brainstem: Sympathetic/Spinothalamic ➡️ S = Side ➡️ lateral syndrome
Hoarseness/dysphagia ➡️ CN 9 & 10 ➡️ medulla (4 cranial nerves in the medulla starting from 12, 4 in pons, 4 above pons)
1
1
10
(3/4) We discussed the approach to diplopia with
@AaronLBerkowitz
@CPSolvers
-> final diagnosis was Tolosa-Hunt syndrome
Join us live next time:
1
1
11
9/
Although rare, intracranial abscesses may be a delayed complication of IE… even after valve replacement & BCx clearance!
For the pt w/ persistent fevers & leukocytosis, low threshold for MRI brain to r/o abscess.
Note, these may present with just AMS!

1
1
10
2/ Migraine attacks may be caused by triggers.
Common studied triggers are alcohol 🍻, sleep disturbances 😴 (either sleeping late, not sleeping or sleeping too much), some types of food 🍽, hormones✨, and emotional stress🤯.
1
2
10
5/
In addition to ischemic stroke, IE may cause cortical SAH & IPH
BOTH may be associated w/ infective intracranial aneurysms (IIAs)!
⭐️ICH in IE = vessel imaging, preferably w/ DSA ⭐️
When to screen for asymptomatic IIA?
Debatable. At least once & ideally also b/f CT Surg

1
0
10
7/ There is still no cure for migraine, but there are many effective treatment options, and a life without recurring incapacitating pain episodes is possible.
1
1
9
🧐References 2/2:

0
5
9
2/
The most common cause of neurologic injury in IE is ischemic stroke.
But! Management is somewhat different.
Notably, due to the high risk of hemorrhagic transformation, tPA is relatively contraindicated or should be used with extreme caution.
You don’t want to end up with ⬇️

1
1
9
If you want to know more about HORNER'S SYNDROME: OR
#ItsAllAboutPupils
episode 4!
Johann Friedrich Horner was a Swiss🇨🇭ophthalmologist. In 1873, one of his students published a thesis describing a woman with "oculosympathetic paresis".
A short🧵containing history and a bit of scientific gossip! 🙊
🧠📚🎨
2
77
242
1
0
9
8/ (1/2) If the patient meets all but one criteria A-D above and does not fulfill other ICHD-3 criteria for any other headache disorder, this person has a probable migraine.
1
0
9
2/ 👀 Visual symptoms are the most common. They occur in over 90% of patients with migraine with aura, are bilateral and can be either positive (scintillations, flashes, etc.) or negative (like scotomas).
1
0
9
(3/3) Review the aura types below ⬇️
Welcome to the
#NeudrawlogyMigraineEdition
, part 2! 🤕🧠
Aura is a Greek 🇬🇷 word and deity that means breeze 🌬, and in medicine, it is a symptom that occurs in up to 25% of people with migraine.
A 🧵! 1/7
#NeuroTwitter
#NeuroTwitterNetwork
#FOAMed
#MedEd
#MedTwitter
🧠📚🎨
2
43
150
1
0
8
Part 3 here:
#NeudrawlogyMigraineEdition
, part 3! 🤕🧠
Migraine is an inherited disorder 🧬of sensory processing with 5 defined phases.
They do not need to occur in every person or even in every attack, and they may overlap.
A 🧵! (1/5)
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd
4
69
235
1
1
9
12/
SUMMARY:Endocarditis
🧠Can present with any number of CNS complications!
❤️Requires thoughtful approach to the timing of cardiac surgery
🧠= Low threshold for neuroimaging.
🦠Necessitates good CNS coverage!
Great reviews:
1
0
9
4/ 🎯 Indications for preventive treatments are (2/3):
- >2 severe or disabling attacks or <4 less disabling attacks per month
- Patient preference
- Highly disabling migraine attacks (e.g., hemiplegic migraine, migraine with brainstem aura)
1
1
9
3/ Ok, now back to the goals.
🎯 Indications for preventive treatments are (1/3):
- Attacks that significantly interfere with patient’s daily routine despite acute treatment
- Ineffective or contraindicated acute migraine treatment
1
1
9
(4/4)
Here you can find the
#tweetorial
about eye movements and gaze palsy!
Hey
#MedStudentTwitter
#neurology
residents,
#EndNeurophobia
#MedEd
#tweetorial
on
EYE MOVEMENTS and GAZE PALSIES
@Tracey1milligan
@MadSattinJ
@CrystalYeoMDPhD
@DxRxEdu
@CPSolvers
@MedTweetorials
8
105
305
0
0
9
Part 5 here:
#NeudrawlogyMigraineEdition
, part 5! 🤕 🧠
Here goes a review of the preventive treatments for migraine! 🧵 (1/10)
✅ Learn here:
🎯 Indications;
💊 General recommendations about the treatment.
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd
#MedTweetorial
5
97
324
0
4
8
13/ NONPHARMACOLOGIC TREATMENT
Neuromodulation: 4 devices are indicated: transcutaneous supraorbital nerve stimulation, remote electrical neuromodulation, transcranial magnetic stimulation, non-invasive vagus nerve stimulation.
1
0
8
6/
The bleeding pattern resulting from ruptured IIA is often NOT the classic “aneurysmal pattern” bleed because unlike CoW aneurysms, IE aneurysms are often:
🎈Found in distal vessels
🎈Small
🎈Fusiform
@alialawiehmdphd
Like ⬇️

1
0
8
Part 4 here:
#NeudrawlogyMigraineEdition
, part 4! 🤕🧠
⏰A migraine attack lasts up to 72h, and can be disabling.
Here goes a review of the pharmacologic 💊 and nonpharmacologic 🏞 treatment of an acute migraine attack🧵! (1/16)
#NeuroTwitterNetwork
#NeuroTwitter
#FOAMed
#MedEd
4
78
234
1
4
7
All the infographics posted so far:
0
3
7
6/ Other recommendations are: (1/2)
- 🪫 Start at a low dose
- ⛔🏃♀️Do not hurry. Some drugs can take four weeks and some up to 6 months to be effective
- 👨🏫👩🏫 Set expectations, explain possible side effects 🤢, and 🥅 goals of care
1
0
7

I am thrilled to share that all my NeuroICU Tweetorials are now indexed on the
@neudrawlogy
website by the extremely talented
@gabifpucci
!
Check out all former
#tweetorial
cases and collect her awesome infographics!

4
42
155
0
2
8
Part 1:
Welcome to the
#NeudrawlogyMigraineEdition
! 🤕 🧠
This first
#infographic
contains the diagnostic criteria for Migraine Without Aura, and in this series, you will see other essential features of this prevalent disease.
🧵 1/10
#Tweetorial
#NeuroTwitterNetwork
#FOAMed
🧠📚🎨
8
120
343
1
2
7
12/ 📚Read more:
Migraine variants in children.
Abdominal migraine: an under-diagnosed cause of recurrent abdominal pain in children
@amfmigraine
1
2
6
4/
In contrast, mechanical thrombectomy does appear to be safe in these patients.
@aneeshsinghalMD
@kellysloaneMD
An example of a septic clot retrieved by mechanical thrombectomy
@emoryneurocrit
@emoryneurosurg
, image from
@feras_akbik

1
0
7
3/ One common visual aura symptom is the fortification spectrum. It consists of zigzag ⦚⦚ lines that gradually enlarges and can either be colored 🌈 or black-and-white 🦓.
1
0
7
⬆️Read/View more! (amazing video included)
0
2
7
4/ Interesting fact: the name fortification spectrum comes from the resemblance to a medieval fortress 🏰.
1
0
6
🧐Although Horner has not claimed the discovery of the syndrome, it became known as his name.
🗺️This is why in some countries it is called Claude Bernard-Horner Syndrome or Bernard-Horner Syndrome.
3
1
6
12/ Remember. Abortive drugs are helpful and safe for use. However, the use of abortives should be limited to < 15 days/month (simple analgesics/NSAIDs) and < 10 days/month (ergots, triptans, others) to avoid the development of medication overuse headache.
1
0
6
8/ (2/2) This occurs because migraine milder attacks or attacks treated early often do not achieve the full criteria, but even though they respond to migraine treatments.
1
0
6
And remember: patients may NOT have diplopia due to severe ptosis!
#FOAMed
#NeurotwitterNetwork
#MedEd
1
1
6
📚The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice.
@ahsheadache
@HeadacheJournal
1
2
6
0
0
6
1/ Like a breeze 🌬 precedes a storm ⛈, the aura usually precedes the headache in up to 60 min.
But not always.
It can also:
- Occurs alone, not followed by any headache
- Occurs during the headache episode
1
0
6
15/ Other options include: resting in a quiet and dark place, hydration, meditation, biofeedback, among others.
1
2
6
5/ Two exceptions:
•Aspirin: irreversibly inhibits COX-1 and COX-2.
•Colecoxib: inhibits only COX-2.
Side effects: gastric ulcer and interstitial nephritis.
#Step1
#USMLE
#Pharmacology
1
1
6