

Andrew Micieli
@MicieliA_MD
Followers
12,837
Following
1,151
Media
448
Statuses
5,659
Stroke/general neurologist @THP_hospital , MINDS clinic. Alum Calgary Stroke Program, @UofTNeurology @SMCS1852 . Author The Code Stroke Handbook; @Neurology_facts
Joined July 2013
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Haitians
• 349679 Tweets
Yunes
• 268874 Tweets
Argentina
• 257561 Tweets
Colombia
• 234358 Tweets
Morena
• 211366 Tweets
PS5 Pro
• 203864 Tweets
Sony
• 140612 Tweets
BTS PAVED THE WAY
• 68459 Tweets
#الكويت_العراق
• 67954 Tweets
Swalwell
• 61172 Tweets
Bolivia
• 54504 Tweets
#TemptationIsland
• 39817 Tweets
Vargas
• 31865 Tweets
Dave Grohl
• 27668 Tweets
Trent
• 27441 Tweets
Barranquilla
• 27090 Tweets
Lola
• 26174 Tweets
#KohLanta
• 20432 Tweets
Fang Fang
• 18254 Tweets
Harry Kane
• 16736 Tweets
Bernstein
• 16466 Tweets
James Rodríguez
• 16111 Tweets
#GHLímite1
• 13663 Tweets
Dibu
• 13583 Tweets
De Ligt
• 12606 Tweets
Alfonso
• 11251 Tweets
#VamosChile
• 10351 Tweets



















Pinned Tweet

🧵Stroke Tweetorials👇🧠💉
by
@MicieliA_MD
Bookmark them for teaching📚.
#neurotwitter
#stroke
#neurology
#MedEd
3
59
201
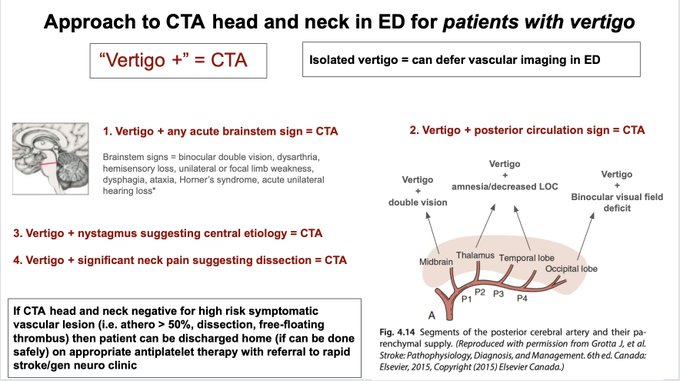
When should you do CTA head and neck in the ED for patients presenting with vertigo?
Below is a "vertigo +" approach to help risk-stratify who can be safely discharged to rapid clinic where further neuroimaging with MRI brain can be considered.
#neurotwitter
#stroke
#neurology
20
214
893
The neurologist seeing that only a non-contrast CT head was ordered for a⚡️thunderclap headache.
#neurotwitter

14
69
726
Pictorial Review of Lesion Localization for Patients With Stroke
via
@GreenJournal
#neurotwitter
#stroke

1
200
636
IT IS NOT A “CVA.” THE PATIENT HAD A ISCHEMIC STROKE. IT WAS NOT AN ACCIDENT…THERE WAS A CAUSE, AND THATS THE JOB OF THE STROKE NEUROLOGIST TO FIND THAT CAUSE.

5
61
393
Here are some key points from
@American_Heart
updated 2022 ICH guidelines:🩸🧠
1⃣ Most common causes: i) arteriolosclerosis ii) CAA (often co-occurring). CAA⬆️recurrence rates
2⃣ Pre-hospital recognition & fast transport important; time =🧠 in ICH
3⃣ CBC, Cr, INR/PTT, tox screen
11
151
376
The stroke neurologist is never fully satisfied with ESUS. Rather than repeating loop recorders they look for:
- occult cancer
- branch artery disease
- aortic arch athero
- non-stenotic extracranial large artery athero
- minor valve disease
- LV wall motion abnormalities
-
11
64
334
CODE STROKE🧠⚡️
Patient is a CT tech at your hospital with witnessed, sudden onset L sided weakness, dysarthria. Stroke neurologist called immediately and assesses patient. NIHSS 15.
Last seen well 10 min ago.
CT & CTP below. Do you treat the patient?
#stroke
#neurotwitter


38
61
315
When to have heighten suspicion for cancer-related ischemic stroke?
- ESUS
- 3-territory DWI infarct pattern
- Smoker (previous or current)
- ⬆️ d-dimer (>3)
- ⬇️ Hgb
- Embolic stroke on DOAC (compliant and correct dose)
#neurotwitter
#stroke


8
97
299
A few tips when performing the NIHSS during a code stroke under time pressure 🧠⏳💉
from The Code Stroke Handbook ()
#neurotwitter
#stroke
#neurology
#medtwitter

4
67
273
Can you name 6 neuroimaging makers of cerebral small vessel disease🩸🧠
Reference
@ContinuumAAN
:
#neurotwitter
#stroke
#MedEd

2
66
240
Door-to-needle time of 17 min today 🧠💉
Key time saving points in acute stroke pathway:
1) through inspection could tell patient had MCA syndrome 2) deferring CTP 3) awesome in-parallel teamwork with EMS, CT techs and nursing team 🙏
#neurotwitter
11
14
241
Updated Canadian 🇨🇦 Best Practice acute stroke management guidelines
update includes TNK💉👇
#stroke
#neurotwitter

3
66
230
“What we currently call core on early CT, CTP or MRI imaging is not actually infarcted tissue but rather a probabilistic estimate of tissue that is highly likely to become infarcted, if fast reperfusion does not occur.”
#neurotwitter
#stroke

10
71
226
You come on service and see this MRI. What is stroke etiology here?
Progress notes are documenting "lacunar stroke"
You take very close look at CTA and see large artery athero in wall of basilar artery.
Etiology here is parent artery plaque (branch atheromatous disease).

14
36
209
Good to know what to do, if you ever run into this situation (as it is often not taught enough in residency)
Regional variation in protocols.
#neurotwitter
#stroke
#MedEd

2
53
180
Thrombolysis is sometimes given for disabling minor deficit (NIHSS 0-4). This is concordant with best practice guidelines.
Pooled analysis shows
- 9.8% mRS 0-1 benefit
- No mRS 0-2 benefit
- 3.7%⬆️ mRS 5-6
sICH🩸rate ~ 2-3%.
Think carefully and don’t

5
37
181

7
26
178
Recent high impact stroke publications/updates:
1. INSPIRES trial via
@NEJM
- DAPT up to 72hr post TIA/minor stroke ()
2. ATTICUS trial via
@NEJM
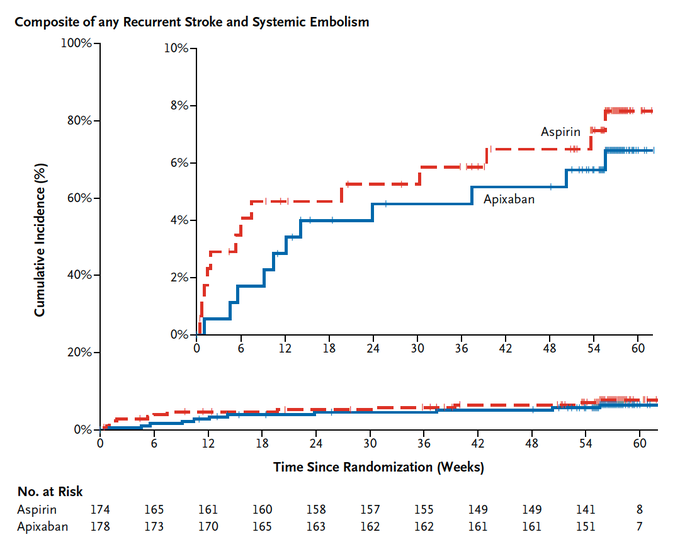
- Apixaban not superior to ASA for ESUS ()
3. Code ICH 🩸 via
@StrokeAHA_ASA

In the ATTICUS trial, among pts w/ embolic stroke of undetermined source and cardioembolic risk factors, apixaban was not superior to aspirin in preventing new ischemic lesions on MRI and was comparable in rates of clinically relevant bleeding.
4
51
140
3
58
179
🧵TIA/minor stroke case🚑🧠
88F presents to ED w/ 30 min of R hand/arm weakness, w/o associated symptoms.
CT/CTA- no signs of early ischemic change and no significant vascular abnormality.
Appropriately started on DAPT, discharged from ED with referral to rapid TIA clinic.
14
39
175
Another good example of how MRI in TIA/minor
#stroke
patients changes management
Patient seen in rapid TIA clinic, MRI ordered and confirms post. circulation DWI lesion but we see this on SWI sequence🩸🧠
This changes antithrombotic & treatment plan going forward
#neurotwitter



8
29
169
Code Stroke 🧠🚑
70s, mRS 2. Wake up stroke, LSW 11:30pm, found 5:30am with dense L sided weakness, dysarthria. NIHSS 18.
Rads report:
CT - ASPECTS 6
CTA- distal R M1 occlusion
Neuro resident "lets go for EVT, ASPECTS 5 so tissue to save"
What do you do? (can't enrol in trial)


22
37
156
You see a white clot removed from EVT. What does that mean?
Case: Young patient presents with aphasia and mild R sided weakness.
NCCT- ASPECTS 10 (no hyperdense sign); CTA shows L M1 occlusion. You give tPA and achieve good recanalization with EVT.
A white clot is removed.


8
39
151
How to risk stratify TIAs.
WHAT an event was and WHY is happened are more important than a score 💯
➡️ Likely reason why some patients benefit more from DAPT (than single antiplatelet)
#neurotwitter
#stroke

2
38
152
Nearing the end of my residency, here is a virtual bookshelf with
#neurology
textbooks I would recommend (& have used) to residents.
Check out the link to the bookshelf which also includes amazon links. Any others you would include?
#neurotwittter
#MedEd

9
15
140
The Code Stroke Handbook.
After 1-yr on the wards & >200 copies sold-- get your copy today at a reduced price. Designed for staff, neuro/IM/ED residents, and medical students covering the entire code
#stroke
consultation.
Links to book below.
#NeuroTwitter
#MedEd
#Neurology


2
18
137
Lets start a thread of practicing changing publications of 2023 in
#neurology
(including all subspecialties) for
#MedEd
.
I'll start with
@TENSIONstudy
in
@TheLancetNeuro
() which showed in large core patients (ASPECTS 3-5) using CT imaging selection, EVT

7
30
133
Really nice summary of TGA just published in
@NEJM
.
I have seen post concussive amnesia, anterior thalamic stroke, or ictal/post ictal phenomena mimic this condition and so often get a MRI brain.
How do others practice?
#neurotwitter
#stroke
#meded

19
32
133
So far in fellowship I've seen thalamic strokes presenting as:
➖ face/arm/leg numbness
➖ patchy arm/leg mild numbness (sparing face)
➖ isolated confusion
➖ full MCA syndrome
➖ MCA syndrome with wrong-way eyes
➖ partial dorsal midbrain syndrome
🤯
#stroke
#neurotwitter
8
8
130
What do you suspect
#stroke
localization/etiology is here?
Radiology reports an infarct in the right basal ganglia and para hippocampus gyrus in the MCA distribution.
CTA is negative for branch artery disease.
Patient presents with L sensorimotor symptoms, L VF deficit

12
22
126
Acute Code Stroke
#neurotwitter
🚑🧠
Help me with this acute
#stroke
decision making.
80 yr old, mRS 0. LSW 5.5 hrs ago. NIHSS >20 (mute, R hemiplegia). CTA shows L distal M1 occlusion, and distal L A2 occlusion. CT/CTA/CTP below.
How would you manage?



16
31
128
If the occlusion is distal to the lenticulostriates then the basal ganglia won’t be affected. An important point I sometimes see overlooked and not factored into acute decision making for distal M1 or prox M2 occlusions
#Neurotwitter
#stroke


1
150
668
1
20
120
Young patient presents as code
#stroke
with left sided very mild weakness/ataxia. This is their second presentation to ED.
CT/CTA/CTP reported as normal. You take close look and see subtle right internal capsule abnormality and suspect a right internal capsule infarct 😏
You


14
22
123
Too many patients seen this week with devastating strokes from holding anticoagulation too long periprocedurally for mild procedures (dental, injections etc) or surgeries.
I think as stroke neurologists we can do better at counselling our clinic patients at each visit, and
9
25
121
Further evidence of benefit of tPA up to 9 hours using CTP, MR perfusion or DWI/FLAIR mismatch from TRISP Collaboration.
#stroke
#neurotwitter

2
25
121
🚨Case where CTP can be helpful🧠
Patient with chronic posterior MCA division
#stroke
, presenting w/ language disturbance & right arm weakness
NCCT: no new ischemic changes
CTA: no occlusion
CTP: left hemisphere hyperemia (⬆️CBF, ⬇️Tmax, ⬆️CBV)
dx: focal seizure
#neurotwitter

6
27
122
An alternative antiplatelet regimen for TIA/minor stroke population is ASA + Ticagrelor for 30d (🇨🇦,🇺🇸, Euro guidelines below)
Consider in patients with high chance of plavix resistance (CYP2C19 loss of function allele)
~15% Caucasions
~30% Middle East, Africa
~60% East Asia



4
33
117
#Stroke
in 2022:
➡️ TNK as routine lytic
➡️ Point-of-care testing for plavix resistance
➡️ MeVO EVT trials
➡️ Mobile stroke units in select cities
➡️ Neuro-protective agents
➡️ Less reliance on CTP
➡️ Better understanding of TNK in minor stroke
to name a few
#neurotwitter
3
19
120
How would you manage a carotid free floating thrombus in setting of TIA/minor stroke?
#neurotwitter
#stroke

18
25
114
CTA is recommended in the ED for high risk TIA/minor stroke patients. It is used to risk stratify patients, who can go home and who needs admission.


@northwoods1980
These changes are likely largely driven by stroke workup guidelines. At least in Canada, concurrent vascular imaging is recommended for any stroke or TIA.

1
0
9
3
40
119
3 tenecteplase RCTs will be presented this week at
#ESOC2022
🧠💉
1⃣
@ActRrct
: pragmatic TNK (0.25mg/kg) vs tPA in Canadian population
2⃣ NOR-TEST 2A: TNK (0.4mg/kg) vs tPA in Norway
3⃣ TWIST: TNK in wake-up strokes vs best standard treatment
#stroke
#neurotwitter
3
25
119
🧵
5 ways to try to be the most helpful inpatient or outpatient medical consultant (neurologist in my case):
1⃣Do not copy and paste the rads neuroimaging report in your note. Give your own concise impression of the report/images. You have the advantage of the clinical details
8
15
118
If you do CTP in early time window you will grossly overestimate core with RAPID rel CBF <0.3.
Why do CTP in early time window? (Except to help with mimics, or trial enrolment)
#stroke
#neurotwitter

5
21
116
🚑Deep dive into nuance of code stroke imaging.
70M code stroke🧠⚡️
Presents to primary stroke centre w/ L MCA syndrome (NIHSS 15), 4hrs from onset. ED calls you to review scans.
CT- ASPECTS 5 (I/L/M1/M4/M5; caudate🤷♂️)
CTA- tandem occlusion; near-occlusion ICA and short


1
32
116
Code Stroke🚑💨
70yr old; mRS 1. Watching TV with family and at end of movie tries to get up and notices R sided weakness, dysarthria. LSW 3 hrs ago.
NIHSS 9.
CT, CTA, Tmax, rCBV 👇. CTA shows L M3 occlusion.
What would you recommend to patient?
#neurotwitter
#stroke
#MedEd


7
23
116

@tmprowell
GBS secondary to COVID is a good example of the significant morbidity associated with the virus, that is not reflected in the media reporting, and when discussing the seriousness of this disease to young (healthy) people. One of many neurological consequences of the virus.
0
13
115
Clinical stem given: aphasic, right sided weakness
You are the neurologist/radiologist
ASPECTS?
#neurotwitter
#stroke

18
22
113
One of the best things in medicine is rounding on a patient who the day before presented paralyzed on one side of the body with severe speech impairment, and after receiving acute
#stroke
treatment is up, walking and talking to you 🧠💉

1
3
111
Every week on inpatient service I see at least 1-2 cancer associated thrombosis. It is common and you won’t find it unless you look. Don’t just call them ESUS then call it a day❌
- ask about constitutional symptoms, have heightened suspicion in certain cases
When to have heighten suspicion for cancer-related ischemic stroke?
- ESUS
- 3-territory DWI infarct pattern
- Smoker (previous or current)
- ⬆️ d-dimer (>3)
- ⬇️ Hgb
- Embolic stroke on DOAC (compliant and correct dose)
#neurotwitter
#stroke
8
97
299
4
36
110
“High-risk TIA/minor stroke patients should be sent for CTA immediately, as half of recurrent stroke events occur within the first 48 hours, many overnight during sleep”
Don’t send a high risk TIA patient home from ED without vascular imaging 😤

8
34
112
Updating the ‘stroke feed’ twitter list for easy access to stroke discussions/threads/pubs/conference updates 🧠💉
#stroke
#neurotwitter
#meded
1
15
106
Stroke clinic is often challenging.
Patient in 60s with PMedHx HTN (on 1 agent), OSA, presents with acute dysarthria.
MRI DWI and SWI 👇. 30-day loop captures very transient atrial flutter/fibrillation.
CTA negative, echo (no atrial cardiopathy). BP and LDL is excellent.


10
14
102
We now have multiple
#stroke
RCTs (ACT🇨🇦, TRACE-2 🇨🇳, ATTEST-2 🇬🇧, TIMELESS🇺🇸) showing the rate of symptomatic intracranial hemorrhage with tPA or TNK is ~3%
Time to move away from the previously quote ~6% from the old RCTs. A likely result of better patient selection and CTA
3
36
102
Excellent review of ICAD
#stroke
by
@CharlesBeaman
@ShadiYaghi2
@dliebesk
ICAD patterns of infarction👇
I often see (C) treated as small vessel disease (lacune) but its branch occlusive disease (BOD) requiring longer duration DAPT (3m)
#neurotwitter

3
28
102
Anyone interested in joining/discussing acute
#stroke
imaging in a future
#twitter
spaces?
If enough interest, could set up a evening discussion on
#TwitterSpaces
#neurotwitter
#MedEd
🧠💉
11
3
100
TRACEIII published (
@NEJM
) showing benefit of giving TNK up to 24 hrs when don’t have access to EVT for LVO
#stroke
#neurology
#MedEd

4
33
99
Stroke case 🏥 🚑💨
Patient in 50s presents to primary stroke centre with disabling left sided sensorimotor symptoms- NIHSS 9.
💉
CT - ASPECTS 9 (insula involvement).
CTA - Right M1 occlusion (thick MIPS and reformats below). Right ICA shows severe stenosis (below)


7
21
97
Every neurology clinic there is a unfortunate patient who had a MRI that wasn’t indicated resulting in the report saying multiple subcortical T2/FLAIR hyperintensities that could be related to headache, demyelination (such as MS) or vasculitis.
Then they wait 6 months to see a

“~15–30% of all diagnostic imaging studies contain at least one incidental finding. Patients with incidental findings but low risk for disease are likely to experience overdiagnosis & overtreatment that create an illusion of benefit while conferring harm.”
49
89
732
6
9
97
Elderly patient presents to hospital with fall and subsequent decreased LOC, L sided weakness, left hemi-neglect.
Notes are documenting the cause of the ICH is traumatic.
Initial CT head, and follow up MRI (SWI seq) 👇
What do you think is main etiology of ICH? Family is


20
20
95
I often see notes imply that the rationale for an echo as part of the
#stroke
work up is to assess for LV thrombus and PFO.
What an echo tells me:
- valvular disease/calcification ()
- ejection fraction; leading to potential DOAC initiation
- regional wall
5
17
87
@DrJacobsRad
I wish my general neurology clinic wasn’t full of long-covid patients. 2023 will be difficult for many
10
4
86
In TIA/minor stroke if MR is negative reasonable to stop DAPT- further evidence from
@JAMANeuro
post-hoc analysis of POINT.
Similar to CHANCE subgroup analysis that benefit of DAPT in TIA/minor
#stroke
is mostly for large artery athero
#neurotwitter

4
21
84
@petrosoniak
@AlexMuccilli
My approach➡️90% is history. Then HINTS + neuro exam. The dx we don’t want to send home is high-risk post circulation stroke.👇 is my approach.
CTA is not used to “diagnosis” stroke but to risk stratify & should be done in select patients.
Interested in your & others approach

5
16
84
Check out our cost-effectiveness paper in
@IntJStroke
showing that if we test for Clopidogrel resistance in TIA/minor stroke and use Ticagrelor in these patients, despite ⬆️cost, ⬆️mild bleeding, patients live longer with NNT of 8 to gain one full QALY

7
26
83
Code Stroke Case🚑🧠
Young pregnant female 10 weeks GA presents to outside hospital with disabling dysarthria, L UMN facial weakness, mild L arm weakness/numbness. NIHSS 6.
Delay at outside hospital and they call stroke neurologist after CT/CTA completed 3.5hrs from LSW.
3
14
82
Here is the recording from the talk tonight
Thanks again to
@a_charidimou
,
@caseyalbin
,
@ShadiYaghi2
.
See everyone next time🧠💉
2
21
82
3
0
81
Advanced code
#stroke
imaging:
Patient presents at 4hours, with mCTA, CTP below.
Predicting tissue fate:
M4 region likely benign oligimia
M5 region likely penumbra
M6 region likely core (infarcted)
Reperfusion therapy with tPA 💉may salvage M5
via
@ContinuumAAN
#neurotwitter

6
16
81
Supporting evidence of low dose tPA (0.6mg/kg) in patients on DOAC (last dose <24hrs).
Would you consider low dose tPA if last DOAC dose 12-24 hrs ago?

5
14
79
Twitter remains a place for
#Neurotwitter
and
#strokeTwitter
to make connections, learn from each others expertise and stay up to date on the latest literature.
Looking forward to what 2023 has to offer 🧠
0
2
79
.
@ActRrct
trial published today in
@TheLancetNeuro
🧠🚑💉
A compelling argument to switch to TNK across 🇨🇦, with its single bolus administration, ⬇️💲, potential ⬆️LVO recanalization
Congrats to
@bijoymenon
@DrRickSwartz
& 🇨🇦 team
#neurotwitter
#stroke



6
22
79

Code
#Stroke
🚑
Patient presents ~1 hr from witnessed onset aphasia + R sided weakness. NIHSS >20.
CT/CTP 👇. L M1 occlusion. Reduced extent of collaterals on single phase CTA.
Radiology reports a large core, ED questions the utility of treatment based on CTP.
What do you do?



21
15
78

20
23
75
No benefit of TNk compared to standard of care for mild (non disabling) stroke presentations with intracranial occlusion/CTP deficit. Definitive answer to this patient population.
@TheLancetNeuro
#stroke
#neurology

2
23
78
Explain this stroke etiology🤷♂️
No branch artery disease and no basilar ectasia.
#stroke
#meded
#neurotwitter


17
12
75
@thebadstats
From a neurological perspective, he fails to mention the potential neurological consequences of getting the flu, or that the flu shot significantly lowers the risk of stroke (across all ages and risk profiles) 💉

4
4
73
How do you manage a patient with a "hot carotid?"
Case:🧠
65M presenting with acute onset of R hemiparesis lasting several hours with resolution who is found to have 80% left-sided extracranial ICA stenosis (no ILT).
Reference: , via
@GreenJournal

3
18
75
Difficulties of diagnosing TIA/minor stroke in clinical practice🧠
Any others?
#neurotwitter
#stroke

2
10
75

Stroke is a horrible disease. As stroke physicians we try our best to prevent/reduce disability and EVT is our most powerful tool. Calgary Stroke Program is leading the way.
Check out this
@nytimes
article by
@evaholland
.
#neurotwitter
4
14
71
Started my
#neurology
residency on-call July 1, 2016 at
@Sunnybrook
.
Ending my residency on-call tonight. Only 12 hours left as a neuro resident 🧠 then off to start my Calgary stroke fellowship 💉
#neurotwitter

5
0
71
Your friendly friday reminder that…
Time is Clot!!⏳🧠💉
tPA resolves clot best when given very early!
#neurotwitter
#stroke

1
19
71
@jeremyfaust
@PenPaperPlanner
Thanks for bringing this to light for the general public.
In neurology we diagnosis PPA (3 subtypes) based on distinctive clues on history and exam (there are diagnostic criteria). It is not a diagnosis of exclusion.
There is the subspecialty of cognitive neurology for this.
2
6
69
@DGlaucomflecken
Don’t say: CVA, EEG to rule out seizures, positive babinski, dysconjugate gaze, do grip strength, give 1g of dilantin 😇
6
1
70
Mark your calendars for an upcoming
@XSpaces
discussion with this ⭐️ panel of
@ShadiYaghi2
,
@a_charidimou
, and
@caseyalbin
.
1
19
68