

M Velia Antonini
@FOAMecmo
Followers
14,136
Following
814
Media
5,529
Statuses
17,798
CCP E-AEC ECMO & NRP specialist + POCUS @EuroELSO Steering C & Chair NRP WG @ELSOeducation taskforce SoMe Director @ELSOOrg SoMe Editor @yourICM @asaiojournal
Italy
Joined February 2011
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
THE LOYAL PIN THAI GL NO1
• 395470 Tweets
#ปิ่นภักดิ์EP1
• 380291 Tweets
Carlos Yulo
• 268132 Tweets
Djokovic
• 260787 Tweets
YOKOFAYE RECAP BLANK SS2
• 115898 Tweets
Rotherham
• 101580 Tweets
ヒロアカ
• 99012 Tweets
Austrália
• 98970 Tweets
エレちゃん
• 96396 Tweets
#tennis
• 82290 Tweets
Kaylia Nemour
• 74646 Tweets
#instagramıGeriVer
• 61747 Tweets
ジャンプ
• 60866 Tweets
Caloy
• 59259 Tweets
SB19 IS LIMITLESS
• 48191 Tweets
Francisca Crovetto
• 44773 Tweets
Bárbara
• 43697 Tweets
最高のヒーロー
• 31593 Tweets
最高の物語
• 31005 Tweets
Nole
• 30076 Tweets
堀越先生
• 26013 Tweets
松山英樹
• 21213 Tweets
松山英樹
• 21213 Tweets
#ありがとう堀越耕平先生
• 21044 Tweets
L1485 FOR LIFE
• 20284 Tweets
Carlitos
• 16353 Tweets
Scottie
• 14881 Tweets
フワちゃん
• 13945 Tweets
#乃木坂工事中
• 12688 Tweets
ジョコビッチ
• 11693 Tweets

















Pinned Tweet

Transesophageal
#ultrasound
guided normothermic regional perfusion in cDCD donors, how we do it: detailed description of technique we use for
#EISOR
(is also worth reading if you use
#REBOA
), just out, open access, on
@asaiojournal
🔓
🖥️ guidewires & EBOA

1
23
55
How to ventilate
#COVID19
pts? Dr Camporota
@Luigi_ICM
shared model to approach reflecting phase of disease during amazing
@ESICM
webinar! hints:
L or H phenotype? (soon on
@yourICM
by
@gattinon
)
#SARSCoV2
pneumonia is NOT
#ARDS
!
#FOAMcc
#SARSCoV2
#Coronavirus
#COVIDFOAM

24
334
523
Pathophysiology of fluid administration in
#ICU
☔️ fluid challenge, bolus, infusion: does rate matter?
💧does type of fluid impact on outcome?
☔️ fluids response in acute circulatory failure: couple macro/micro hemodynamics
#FOAMcc
on
@ICMexperimental
🗞️

2
140
351
#COVID19
dedicated
@GiViTI_IRFMN
@MarioNegriIRCCS
video conference with intensivists from North of Italy sharing their initial experience with
#Coronavirus
#SARSCoV19
epidemics: LUS, proning, MV
#ECMO
... it's like a tsunami, you can't understand if not in
#FOAMcc
#FOAMed
#FOAMus

15
278
348
Managing critically ills
#COVID19
pts? be prepared! be familiar with case definition, strict compliance with IPC
@ESICM
webinar by Prof
@YaseenarabiYa
with
@Lennie333
Here my graphics, slideset & summary by
@WhistlingDixie4
at
#FOAMcc
#FOAMed
#Coronavirus

1
198
286
MV is like recipe: same ingredients/different dosages may result in perfection vs disaster
Low Vt does NOT guarantee lung protection: could be good starting point, but isn't THE solution, scale to lung size. Vt impacts survival (ARMA) only if really high/low
@Luigi_ICM
#LIVES2020




5
98
279
Advices & informal algorithm by intensivists daily caring for pts w
#SARSCoV2
in Milan, to stardardize approach optimizing outcome & resources consumption, & support HCPs dealing with severe
#COVID19
resp failure
by
@Thom_Langer
@Bottinik1
graphics
@FOAMecmo
#FOAMcc
#COVIDFOAM

8
154
276

🚑 Inside the mobile
#ECMO
truck of MN Mobile Resuscitation Consortium providing
#ECPR
in refractory
#OHCA
in Minneapolis, equipped to allow for echographic/fluoroscopy guided cannulation on the road
@MMRCbeat
@DYannopoulos
#PraguECPR
12
85
261
Prone position for acute hypoxemic respiratory failure &
#ARDS
, a review:
➡️ physiologic features: ventilation & perfusion
➡️ clinical outcomes
➡️ awake prone positioning
➡️ practical considerations
➡️ lingering questions & future directions
@accpchest
🖇️

0
104
249
Everything about fluids
@Manu_Malbrain
#IFAD2020
🔹7⃣Ds & fluid stewardship
🔹(fluids related) definitions
🔹4⃣questions
🔹4⃣indications
🔹4⃣phases & ROSE conceptual model
🔹fluids myths
🔹main references
Graphic
@FOAMecmo
#FOAMcc
Full talks available at

6
99
242
Ever experienced membrane lung failure on
#ECMO
??
📌 mechanisms of ML (function &) dysfunction
📌 ML monitoring
📌 algorithmic approach to troubleshooting
@Crit_Care
#FOAMcc
#FOAMecmo
So proud being among authors
*Hint: do NOT miss supplementary info!

4
84
241
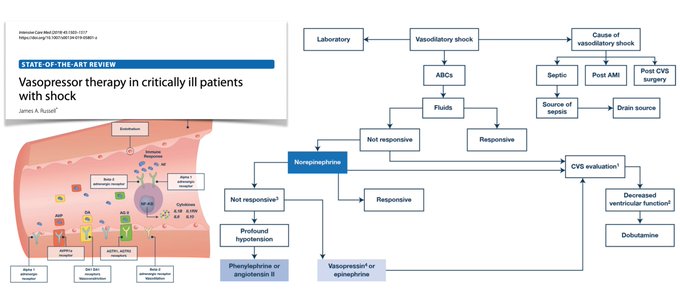
Vasopressors in shock
➡️norepi 1st choice in septic/vasodilatory shock after volume
#resuscitation
, may be followed by vasopressin/epi
➡️angiotensin II/dopamine limited indications
➡️may ⬇️contractility: inotropes may be added, dobuta>milrinone
@yourICM


Vasopressors in critically ill pts with shock:
➡️summary of evidence & pivotal trials
➡️relevant pathophysiology of vasodilatory shock
➡️when & what vasopressor(s) to administer? agents & receptor/effect(s), dose, additional benefits
➡️monitoring
➡️weaning
3
264
531
1
90
240
Serum lactate poorly specific for hypoperfusion, more often associated with impaired tissue O2 use. Levels affected by
⬆️ increased anaerobic glycolysis & ⬆️ aerobic glycolysis production
⬇️ impaired mitochondrial function
⬇️ reduced hepatic clearance
Potential harm may result

Guiding resuscitation on serial lactate measurements? Not an accurate biomarker of hypoperfusion. However integration with clinical phenotyping + peripheral perfusion assessment could better individualize strategies
🔓
Refers to
🔓

2
66
180
0
112
238

Acute RV injury in surgical & critical care settings
🔗
🫁 acute respiratory distress syndrome
#ARDS
🧫
#sepsis
& septic shock
🟤 liver disease &
#transplantation
🫀 management of RV Injury & Failure
#ThePeoplesVentricle
🫀 2 just out on
@JCVAonline
Also

2
91
230

Basic
#echocardiography
infograph based on
@ESICM
#LIVES2019
masterclass! you are captain of the ship, manipulate probe on chest till you find good acoustic window but do not pretend to do full echo study, learn basis first
#FOAMus
#POCUS
graphic
@FOAMecmo
scans
@Wilkinsonjonny

7
117
217
Hemodynamic management in
#COVID19
notes based on A Messina talk
@HumanitasMilano
@ESICM
webinar Start from clinical examination, add
#POCUS
to basic monitoring (ie PPV), complex tools in selected cases only
#COVIDFOAM
video
slides

2
124
212
🌡️Fever
1⃣ measure t° accurately
2⃣definitions vary
3⃣diagnostic workup? only in some pts
4⃣consider non‑infectious causes
5⃣treat MH
6⃣7⃣8⃣ sepsis? careful w control; NO fever? NO good sign; paracetamol/cooling doN'T ⬆️ outcomes
9⃣BI?
🔟 control post CA
🔗

0
85
211
Acute RV injury in cardiothoracic surgery &
#ICU
, 1
🫀 cardiac surgery: CPB/myocardial protection, RV afterload, RV ischemia
🫀🫁 heart & lung
#transplant
🫁 chronic thromboembolic PAH
🫀
#LVAD
🫁 thoracic surgery: one-lung MV/lung resection
@JCVAonline
🔗

3
88
205

Delayed fluid therapy can lead to ischemic injury, irreversible shock with multisystem organ system; here 10 papers we should know about
#resuscitation
fluids:
#IFAD2020
Rodriguez G
1⃣CRISTAL RCT
@JAMA_current
2⃣SAFE Study
@yourICM




2
79
200
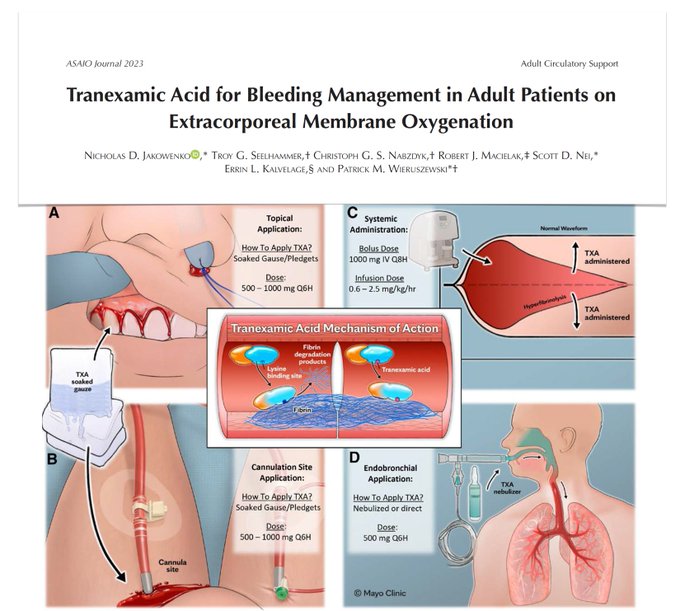
Topical, nebulized, endobronchial, systemic tranexamic acid to manage surgical & medical bleedings on
#ECMO
🩸TXA commonly used as adjunctive hemostatic agent
🩸systemic TXA use low, guided by local protocol involving multidisciplinary approach & rigorous VET monitoring
0
71
193
Evaluating volemic status & fluid management
@DrMCecconi
#eSMART2021
tutorial 🧵
🩸vessels: elastic compartment, fluid filled (blood)
🩸Unstressed Volume: fluid not generating stress on vessels walls
🩸Stressed Volume: fluid generating stress = Pressure = mean systemic filling P

1
83
190




Why measuring respiratory drive & effort in
#ARDS
??
➡️high breathing effort? ➡️ lung stress/strain + diaphragm injury
➡️monitor effort at bedside (ie Pes, P0.1, EAdi)
➡️prioritize lung vs diaphragm protective MV
@DrLeoHeunks
#eSMART2021
📰 PS read
@yourICM




1
77
190


Why to assess preload responsiveness?
💧NOT all pts even in shock are fluid responsive
💧assess frequently: dynamic phenomenon
💧fluids in non-responders? risky
💧overload harmful: +ve balance ⬆️ mortality
💧use of fluid responsiveness tests ⬆️ outcome
Teboul JL
@ESICM
webinar 🧵




1
57
182
Lung ultrasound in acute & chronic heart failure
🖥️ findings: B-lines, pleural effusions & other
#POCUS
features of congestion & deaeration
🖥️ LUS technique
🖥️ clinical applications: diagnosis, monitoring, prognosis & follow-up
🖥️ integrated cardiopulmonary
#ultrasound
🖥️ gaps in

1
95
182


Understanding gas analysis
#eSMART2021
tutorial 🧵Starting from oxygenation:
🩸O2 content Hb bonded + dissolved in plasma
🩸lung capillary? assume Sat 100%; calculate PAO2 alveolar PO2 with alveolar gas equation
🩸enough Hb? CaO2 may be preserved despite low PaO2/SaO2
@Luigi_ICM

2
73
173
Essential of lung/diaphragm
#POCUS
tutorial 🧵
🦇 sign identify lung in ICS (ribs acoustic shadows)
__ pleural line moves w ventilation: visceral/parietal pleura sliding
🅰️ lines horizontal reverberation artifacts similar to pleural line (repeats = distance)
Mongodi S
#eSMART2021


4
63
169
Temporary Mechanical Circulatory Support in refractory cardiogenic shock
♥️ definition & medical management of CS
♥️ overview of devices used in CS
♥️ escalation of tMCS
♥️ management of tMCS in
#ICU
♥️ de-escalating/weaning
@AHAScience
#FOAMcc
#FOAMecmo
📎

2
65
169
Heart-lung interactions in pneumonia
@ESICM
webinar: De Backer D moderated by
@Echotrainer
basic physiology
#ARDS
&
#COVID19
acute cor pulmonale
fluid status/responsiveness (& assessment)
slides + high res graphics
#Coronavirus
#COVIDFOAM
#FOAMcc
#FOAMus

6
91
168

Before giving fluids, consider:
🔹is CO too low?
🔹should I give fluids?
🔹obvious fluid losses?
Fluid overload is harmful, negatively impacting on prognosis; moreover, effects of fluid infusions are not constant ➡️ assess responsiveness/unresponsiveness!
@PrXaMonnet
#IFAD2020




2
52
157

Oxygenation on VA
#ECMO
, review aimed to highlight physiology, summarize current data reporting association with outcomes & outline an approach to titrate O2
@CritCareMed
📎
🫁complex determinants of systemic oxygenation: key circuit & patient factors

2
71
158
Fluids in sepsis?
💧adaptative to retain H2O/Na+ & ⬆️ lactate
💧few pts have lost/loose fluids
💧most fluids in
#ICU
drugs/nutrition
💧first 30 ml/kg standard care, probably OK in most, then bolus if marked hypoperfusion, stop if no improvement/⬇️ oxygenation
@AndersPerner
@ESICM




5
50
156
Missed
@ESICM
#COVID19
webinar with Professor Bin Du from China? here notes on
#Coronavirus
pandemic, clinical features, organ failure, need for mechanical ventilation; check ESICM blog &
@WhistlingDixie4
thread for more data!
#FOAMcc
#FOAMed
@ecmocard
@CCRG_Research
@APELSOorg

5
115
153
Veno-Pulmonary Arterial
#ECMO
in severe
#ARDS
, all you need to know in this editorial!!
⚙️ physiology
📖 evidence
🫀🫁 VPA
#ECLS
&
#ARDS
cardiorespiratory phenotypes
🔮future
@asaiojournal
@prorvnet
#ThePeoplesVentricle
🔓Just out open access
#FOAMcc
at
📖

1
71
154
Still a place for old monitoring tools in the
#ICU
?? 1/2
📌 what is the problem with CVP? CVP does not tell us about fluid responsiveness, but we may still use for something else... about preload/right heart, so we should measure it!!
@PrXaMonnet
#IFAD2020
@Fluid_Academy
#FOAMcc




6
63
150
Venous Excess UltraSound?? window on venous (congestion) pathophysiology, which might guide precise fluid management! Here conceptual review + case series focused on
#VExUS
grading system: pathological basis, pitfalls, limitations
#FOAMus
#echofirst
#POCUS

0
64
152

About significance of EtCO2 & how it relates to PaCO2, notes based on
@gattinon
talk at
@Smart_Meeting_M
2018... back to physiology here! Waiting for
#SMARTmi2019
full talk open access at
#FOAMcc
#FOAMed
follow the hashtag and see you next May in Milan!



3
80
149
Head-to-toe bedside
#ultrasound
for adults on
#ECMO
🔓
🫀🫁 prior to ECMO initiation: echocardiography, indications-contraindications + choice of configuration, pre-cannulation findings, LUS
🚨
#POCUS
during
#ECPR
🖥️ procedural guidance: vascular access

0
66
147
🫁 🫀 Right ventricular injury in the setting of hypoxemia, hypercapnia, elevated RV afterload may impact on mortality in
#ARDS
on VV
#ECMO
: protecting RV to improve survival?? Cardio/(pulmonary) vascular physiological considerations on
@asaiojournal
🖇️

2
50
150
Perfusion pressure is not exactly MAP: look at both sides of circulation: venous (dark side) of circulation need some attention! how much congestion is affecting organs??
VExUS Venous Excess
#ultrasound
@ThinkingCC
#COVID19POCUS
#POCUS
#echofirst
#FOAMus




2
79
145
Ventilator settings in
#ICU
: prioritize permissive over aggressive ventilation!
1️⃣ use low Vt
2️⃣ do not use high PEEP by default
3️⃣ check delta P & MP
4️⃣ reduce RR
5️⃣ use O2 wisely
6️⃣ integrate
Schlultz M
Utrecht 🇳🇱🫀🫁
@ESICM
#LIVESforum
#FOAMcc


👇👇👇Great summary on how to set the
#ventilator
in critically ill patients - 6-step approach in
#mechanicalventilation
✍️ Marcus Schultz
#LIVESFORUMUTRECHT

1
24
76
0
72
144
Our
@ELSOOrg
guidelines for adult & pediatric
#ECMO
circuits:
⚙️cannulation sites & cannula selection
⚙️circuit composition
⚙️tubings
⚙️membrane lung
⚙️blood pump
⚙️priming
⚙️monitorings
⚙️coming off emergently
Just out on
@asaiojournal
open!!
#FOAMcc

5
57
144
HFNC in acute resp failure: what guidelines say?? recommendations on
@yourICM
➡️hypoxemic failure STRONG
➡️peri-intubation NO
➡️post-extubation CONDITIONAL
➡️postop CONDITIONAL high risk/obese
@Bram_Rochwerg
#ESICMwebinar
Also read




0
60
144
Diaphragm main respiratory muscle: dysfunction frequent/impactful in critically ills
How to assess? diaphragm
#ultrasound
1 diaphragm excursion
2 diaphragmatic thickening/thickening fraction
#DUS
in
#COVID19
? non critical/critical pts NIV/IMV Boero E
#COVID19POCUS
#POCUS
#FOAMus




2
76
143


Surviving Sepsis Campaign guidelines on
#COVID19
critically ills management in one visual abstract
IPC
hemodynamics
Non-Invasive/Invasive ventilation
therapy
check post on
@ESICM
blog for high resolution pics/full text link
#coronavirus
#SARSCoV2
#FOAMcc



8
77
137
New global definition of acute respiratory distress syndrome
#ARDS
@ATSBlueEditor
Intubation? not required
💨 HFNO ≥ 30 L/min or NIVICPAP ≥ 5 cm H2O PEEP
🫁 hypoxemia: Pa02/Fi02 ≤ 300 mmHg or SpO2/Fi02 ≤ 315 mmHg with SPO2 ≤ 97%
☢️ 🖥️ bilateral opacities confirmed by: CXR,


New ARDS definition🫁
What's new👇
1⃣HFNO ≥30 L/m
2⃣SpO2/FiO2 ≤315 & SpO2 ≤97
3⃣Ultrasound diagnosis of bilateral opacities
4⃣Consideration for resource-limited settings
But it's hard to know the consensus process from one-page abstract🤔
🔗
#FOAMcc

29
501
1K
3
65
135
How to manage differential gas
#ECMO
??
🫀 mechanism of dual circulation
🫁 impact of dual circulation on gas exchange in different regions of the body
🟥 lack of competitive flow, no dual circulation
🟦🟥 dual circulation with impaired native gas exchange
🟥🟦 dual circulation

0
54
131
#ECPR
vs prolonged conventional ACLS only in refractory
#OHCA
⬆️ survival
⬆️ favorable neuro-outcome
secondary analysis of Prague OHCA trial 🇨🇿
⚡️⏳⏱ Better survival if initial shockable rhythm, younger age, shorter
#resuscitation
@Crit_Care
#FOAMcc
🖇️

1
65
130
What an honour! My drawings showing recirculation on VV
#ECMO
featured on cover page of new issue of
@asaiojournal
!! This graphic is among the illustrations included in
@ELSOOrg
guidelines for
#ECLS
circuit in adults & pediatric pts, free open access at
🖇️

9
17
129

How to unload left ventricle during VA
#ECMO
??
🖥️ echocardiographic imaging protocol
#POCUS
🖥️ aortic valve, ventricular size & LAP
🖥️ LV unloading device selection
Open access
#FOAMcc
#FOAMus
#echofirst
@ESC_Journals
@escardio
🔓

1
60
130

Cannulation configuration & limb ischemia-related complications on peripheral VA
#ECMO
in adults,
@ELSOOrg
Registry analysis on
@CritCareMed
➡️ bilateral cannulation should be preferred approach if femoral cannulation
🖇️
📊 > 19K patients, about 12k

0
56
128
EXODUS, EXpert consensus On Diaphragm
#UltraSonography
in critically ill
🔓
Evidence-based statements on:
⚙️ diaphragm anatomy & physiology
🫁 ventilator impact in diaphragm
#POCUS
🖥️ transducer settings & technique
🎓 learning & expertise
🩺 applications

0
53
127

#POCUS
to assess volume status/manage fluids? Volume is NOT preload, fluid responsiveness does NOT mean give fluids: assess fluids tolerance!
🫀 right: IVC/RV size, portal/renal flows
🫀 left: MV inflow pattern, LA size, IAS, B lines
@iceman_ex
#LIVES2022




2
40
126
How to assess diaphragm with
#ultrasound
??
➡️ visualize diaphragm, hyperechoic line (left: use splenic window)
➡️ M-mode, 2/3 regular breaths
➡️ measure excursion; shallow breaths > 1 cm m/> 0.9 f
➡️ measuring shortening fraction feasible, not so easy
B Cholley
#LIVES2022
#POCUS




3
40
127
🦋 Brain
#ultrasound
? NOT only in neurocritically ill but also in general
#ICU
ie after cardiac arrest or
#sepsis
4 windows
🪟 temporal (major)
🪟 submandibular (carotid)
🪟 optical (linear probe for OSND)
🪟 suboccipital (vertebral/basilar)
#LIVES2022
@chiara_robba
@aartisarwal




0
58
125
Do you think you know anything about edema? to fully understand edema formation take a look at this infograph based on Pietro Caironi talk at
#IFAD2018
meeting
@Fluid_Academy
#FOAMcc
#FOAMed

1
86
126

Everything you need to know about (periop)fluid physiology, infograph based on Robert Hahn talk at
#IFAD2018
meeting
@Fluid_Academy
#FOAMcc
#FOAMed

0
79
124
7 principles of Lung Ultrasound in Critically Ill
#LUCI
() &
#echo
diagnosis of lung consolidation Lichtenstein D masterclass at
@ESICM
#LIVES2019
take home message? fractal sign: non translobar vs lung sign: translobar
#FOAMus
#FOAMed
#POCUS
#echofirst

1
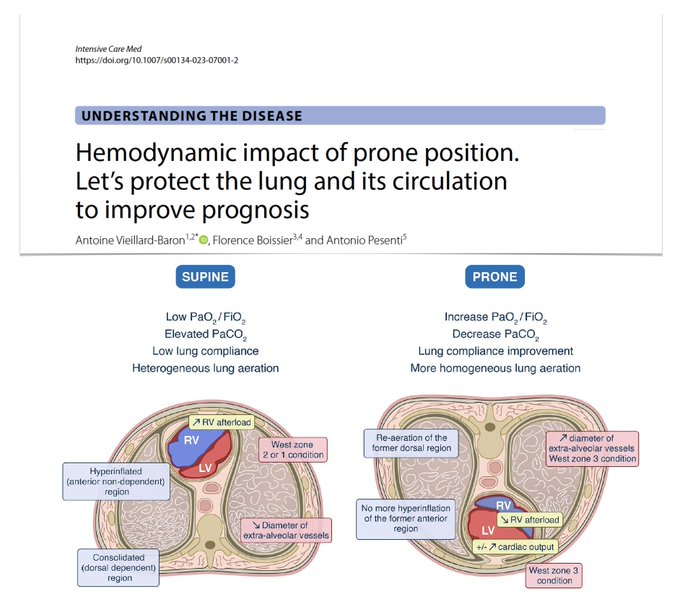
74
124
🫁 Hemodynamic impact of proning? Let’s protect lung & its circulation to improve prognosis! RV to be evaluated in supine position before/after turning prone ARDS pts if overload? Could RV failure be itself be an indication for PP, whatever blood gases?
🖇️

🫁 Let’s protect lung & its circulation to improve prognosis! Besides limiting VILI/improving oxygenation, proning protects pulmonary circulation, unloads RV, improves hemodynamics, maybe partly explaining its beneficial effect especially if RV failure.
🖇️
4
157
410
0
42
122
Everything you need to know about fluid therapy:
📌fluids are not innocent
📌fluids are not just bag of water
📌fluids should be treated as drugs
📌fluids status matter: hypovolemia is bad, overload is worst!!
Always consider 7 D's ➡️ fluids stewardship!
@Manu_Malbrain
#IFAD2020




0
53
121
AKI &
#COVID19
: common in ICU patients (30–50% incidence);
#AKI
marker of disease severity & negative prognostic factor for survival.
#RRT
Renal replacement therapy is required in 10-20% of ICU pts with
#SARSCoV2
infection
Schneider A
@ESICM
#ESICMwebinar
#ESICMtv
#COVIDFOAM



2
69
119
#RESUS21
new
@ERC_resus
guidelines
🫀ACLS priority? high quality compressions/minimal stops early defibrillation, treating reversible causes
🫀consider rescue
#ECPR
(selected pts) if ALS fails or to facilitate procedures
PS look at special circumstances CA




0
65
121
Efficacy of IV fluid administration & potential harm from fluids
#resuscitation
: complementary strategies may
be used to prevent & treat overload: restrictive admin + active removal, look at ROSE model
@Manu_Malbrain
@Fluid_Academy
open
#FOAMcc
#FOAMed

1
77
122
🩸 Anticoagulation in
#ICU
: search for safer anticoagulants continues! Bleeding & thrombosis main cause of morbidity & mortality on short-term percutaneous mechanical circulatory support as
#ECMO
,
#IABP
,
#Impella
, due to interplay of factors influencing haemostatic balance,


0
37
120
Using
#ultrasound
(& not only) to assess cardiac preload & fluid responsiveness
@PrXaMonnet
how to, advantages, drawbacks/limits & evidence of
fluid/mini fluid challenge
PVV/SVV
ΔSVC/IVC
recruitment
EEO/EIO
PLR
full talk
#FOAMcc
#FOAMus
#POCUS
#echofirst



0
55
119
Understanding acid-base and beyond, Thomas Langer at post
#IFAD2018
course
@Fluid_Academy
#FOAMcc
#FOAMed

4
79
118
Do NOT miss on acute RV injury in surgical & critical care on
@JCVAonline
1️⃣
🫀🫁 cardiac & thoracic surgery
🫀🫁 heart & lung
#transplantation
🫁 chronic thromboembolic PAH
🫀
#LVAD
2️⃣
🫁
#ARDS
🧫
#sepsis
& septic shock
🟤 liver




0
45
114
In
#COVID19
you may have severe hypoxemia with low recruitability; as consolidation increases with increased compliance/recruitability, treatment of same patient with same pathology & same degree of hypoxemia need to be adjusted (tailored) accordingly
@Luigi_ICM
@ESICM
#LIVES2020




3
45
119
Gastrointestinal failure & injury in
#ICU
?? We do not have proper definition of enteral feeding intolerance: consensus process needed, potentially leading to proper therapy. But how to define enteral function & GI dysfunction? Concomitant symptoms important!
🍽️ 1 symptom in pt




1
54
118
Weaning from VV
#ECMO
➡️ V’O2ML
➡️ V’CO2ML
⬇️ effects of reducing EBF
⬇️ effects of reducing SGF without altering FdO2
⬇️ effects of reducing FdO2 prior to reducing SGF
➡️ patient
➡️ ventilator
➡️ proposed (physiology based) approach
@ICMexperimental
🖇️

0
47
116
Extracorporeal CardioPulmonary Resuscitation
#ECPR
response team: how physicians implements prehospital
#ECMO
on the streets of Paris
#ECLS
#ECPR
@LionelLamhaut
@alice_hutin
photos
@samudeparis


2
81
116
Theoretical distribution of intravenous fluids on infusion?
consider
🔹1 lt "NS"/balanced crystalloids? ➡️ 820 ml go to interstitial/lymphatic space
🔹1 lt G5%? ➡️ 600ml go to IC space
🔹hypotonic NaCl/G4% ➡️ 480ml IC
check
@bmj_latest
Nijsten M
#IFAD2020



1
46
116
VA
#ECMO
, knowledge gaps
1️⃣ indications
2️⃣ selection criteria for
#ECPR
3️⃣ cannulation: percutaneous vs open
4️⃣ therapy goals
5️⃣ BP & vasoactives, less is more?
6️⃣ transfusions
7️⃣ anticoagulation
8️⃣ endothelial activation/damage
@ICMexperimental
#FOAMcc
🗞️

0
62
116
How to write a meaningful paper (& get it published)? Prof M Slaughter
@asaiojournal
EiC
#ELSO2023
The 3️⃣ Cs
🎯 Clarity of the message
🎯 Cohesion
🎯 Conciseness
Common reasons for rejection
➡️ general: topic not of sufficient interest to readership, manuscript does not conform




1
45
112
10 tips to manage severe acute pancreatitis in
#ICU
#FOAMcc
on
@yourICM
@JABERSamir3
🖇️
1️⃣ Identify patients at ⬆️ risk
2️⃣ admit if organ failure
3️⃣ identify etiology
4️⃣ early abdominal CT to exclude differential diagnoses
5️⃣ monitor IAP (bladder P)


2
43
112
#Extracorporeal
CPR in cardiac arrest
@DYannopoulos
presenting Minnesota experience, recent launch of University of Minnesota's
@UMNews
mobile
#ECMO
program & ARREST trial.
Main effect of time (CA to
#extracorporeal
reperfusion) on survival/outcome!
@escardio
@EuroELSO
#ACVC2021




1
50
113
MV setting guided by waveforms mandatory skill in ICU; as asynchronies are frequent associated with inappropriate treatments/poor outcomes... do not wait them to occur!! Mojoli F at
@Smart_Meeting_M
2018 waiting for
#SMARTmi2019
full talk
#FOAMcc
#FOAMed



1
72
115
Mannitol vs HTS in intracranial HT?
osmotic gradient ➡️ brain dehydration
⬇️ blood viscosity ➡️ cerebral vasoconstriction ⬇️ ICP
hypertonicity ➡️ CSF reabsorption
⬆️ ICP + edema use HTS
monitor electrolytes/osmolarity
@NeurocritCareJ
@drdangayach
#IFAD2020




1
48
113
#ECMO
in
#COVID19
, updated
@ELSOOrg
guidelines:
📌program
📌pt selection
📌cannulation & ongoing care
📌weaning/discontinuation
#ECLS
in
#PedsICU
@JenelleBadulak
@stead_christine
@GraemeMacLaren
@kshekar01
among authors, proud to be one!
open
@asaiojournal

3
55
110
One of major advancements in ARDS? understanding
#ARDS
strictly related to concept of baby lung: MV injurious in ARDS due to ⬇️ lung size inflated by Vt
Dynamic strain (impacting on VILI/outcome)? Vt/FRC
Compliance most close FRC estimate (NO PBW)
@DomGrieco
@ESICM
#ESICMwebinar




1
44
108

⏱️
#ARDS
? First 24 h = “golden” period which should be time stamped:
1️⃣ 🔍 first 3h of non-invasive/invasive respiratory support: rule in ARDS diagnosis
2️⃣ ⚖️ first 12h: decide to continue NIV or institute IMV
3️⃣ 🫁 first 6h: implement low Vt strategies & optimization based on

1
41
111
