

Andrew Sanchez
@ASanchez_PS
Followers
8,219
Following
1,665
Media
844
Statuses
6,429
Hospitalist @BIDMC_IM Teaching/Learning Dx❓, Co-host @Dx_Atypia (Winter '24) 🎙, @CPSolvers Academy🕵🏽♂️, @YaleIMed @ColumbiaPS @UF 👨🏽🎓
Boston, MA
Joined May 2009
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
FEMA
• 477279 Tweets
Mutombo
• 217798 Tweets
Mets
• 164588 Tweets
Verizon
• 121614 Tweets
Pete Rose
• 105964 Tweets
Braves
• 97087 Tweets
Lions
• 54913 Tweets
#WWERaw
• 45063 Tweets
Hall of Fame
• 35507 Tweets
Titans
• 31972 Tweets
Dolphins
• 30152 Tweets
WELCOME HOME BAMBAM
• 27561 Tweets
Seahawks
• 23501 Tweets
#ラヴィット
• 22313 Tweets
あと3ヶ月
• 18400 Tweets
Hit King
• 17292 Tweets
コーヒーの日
• 17207 Tweets
Happy New Month
• 17171 Tweets
愛知1区
• 13735 Tweets
#SnowManライブグッズ
• 13353 Tweets
Will Levis
• 12510 Tweets
残り3ヶ月
• 11844 Tweets



















Pinned Tweet

📌 See below for my collection of:
- Tweetorials for Diagnosis❓
- Case Challenges❗️
-
@CPSolvers
Presentations ♥️

3
10
63

How I teach students & interns on rounds without 📜 & ✒️:
1) "You'll get an email summary at end of the day. Feel free to not take notes!"
2) Verbal teaching 5-10 minutes
3) Send durable educational resource vs. new, free-form bulleted teaching via email! I usually do both!


25
228
1K

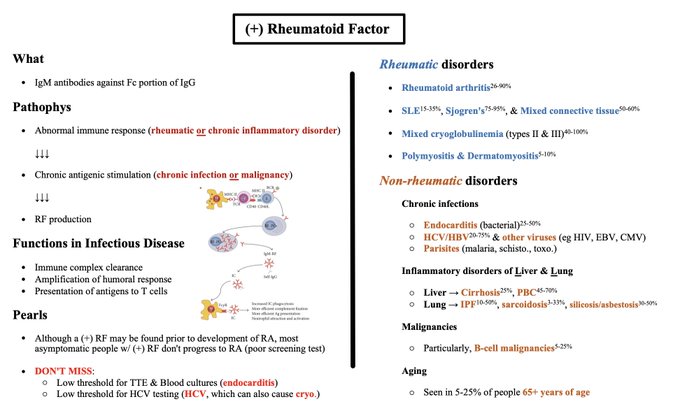
Approach to a (+) Rheumatoid Factor (RF)!
As we've all heard, RF is poorly named because (+) RF does not always = RA.
So, what is RF?
9
235
831
Everything "Aspiration Pneumonia" for the incoming IM interns 🤮🫁:
3 major types of aspiration sequelae!
🫁 Mechanical obstruction (straightforward)
🫁 Chemical pneumonitis ("aspiration pneumonitis")
🫁 Bacterial aspiration pneumonia (*true* pneumonia)
1/x

8
225
810
🔥 Schema for New Fever in the ICU 🔥
~50% infectious
~50% non-infectious
The schema starts at the head/neck & ends at the toes (extremities)!

5
193
654
🫁💧 Pleural Effusion Schema 💧🫁
1) Thoracentesis → Calculate Light's criteria (Note: ~20-25% of true transudates are misclassified)
2) Stratify transudative DDx by Starling equation (Hydrostatic, Oncotic etiologies) & Diaphragm-related etiologies
3) Exudative DDx = longer!

7
189
641
🫠 Approach to Hypotension 🫠
Recent ICU shifts = newfound appreciation for this clinical dilemma.
The traditional breakdown of hypotension/shock is very classic: my schema aims to sub-divide this framework & cover some new buckets.
Read on! 🧵

8
171
566
💥 Monoclonal Gammopathies of Clinical Significance! 💥
Everyone knows MGUS.
Monoclonal proteins are simply blameless protein markers until clonal B-cells progress to Myeloma, Waldenstrom's, or another disorder, right?
...It turns out, not quite!
Let's explore!

9
184
544
Schema for 🎆Thrombotic Microangiopathies (TMAs)🎆
How do you arrive here?
(1/x)

1
151
516
😵💫 Approach to Dizziness! 😵💫
4 big buckets:
- Pre-syncope
- Vertigo
- Imbalance/Dysequilibrium
- Psychiatric
This approach is very much a bird's eye view approach that should assist in history/data acquisition. I'll also cover a tricky don't-miss Dx.

3
120
513
Approach to Cytopenias, frameworks from:
@AndreMansoor
@MatthewHoMD
@tony_breu
@AaronGoodman33
@CPSolvers
@rabihmgeha


3
151
486
🫀 Approach to HFpEF Dx 🫀
I loved creating this one-pager because my understanding of how to clinch this Dx shifted enormously throughout my intern year.
Turns out, "no diastolic dysfunction" on TTE doesn't = no HFpEF.
Let's go through the pathophys & see how this assists Dx.

10
134
439
🦀 Approach to Lymphomas 🦀
Re-sharing this updated framework with some increased organization, new references, & more specific terminology.
Let's take this ride again!

8
91
386
💀 Pulmonary Infarction 💀
Is that focal chest consolidation a pneumonia? 🤔
Let's talk about a pneumonia mimicker that can be *very* easily missed if you've never seen it before 🎭

9
118
377
💥 Approach to Elevated Tryptase 💥
A patient without a history suspicious for anaphylaxis or angioedema presents with an elevated serum tryptase.
How do we interpret this uncommonly sent lab test?

8
86
343
Frameworks, Schemas, & Algorithms for Internal Medicine
2
84
324
🟤 Approach to Acute Hepatocellular Injury 🟤
The DDx of ↑ AST & ALT out of proportion to ↑ in cholestatic labs is easy for most.
BUT! I think some can't-miss conditions are frequently left out by early learners.
Here's a diagnostic approach that'll prioritize those causes.

6
95
331
I'm thrilled to announce I accepted an academic hospitalist position at
@BIDMChealth
!
A huge thanks to HMED chief Joe Li for working with me to craft this dream job. This decision couldn't feel more right.
@LaurenEFields2
, I'm coming to Boston!

49
13
323
Framing lymphomas for clinical reasoning: a Herculean task given long list of diseases in our world of molecular biology.
Here's my first attempt at a summary:
1/11

5
73
324
☠️ Approach to Ischemic Limb Syndromes ☠️
You're in the ICU examining a patient & find a patient with purple discoloration of an extremity concerning for limb ischemia
But the patient *has* distal pulses!
What's going on? 🧐
Take a journey with me &
@OmarosisFugax
!

7
132
325
🩸 Framework for Platelet Disorders 🩸
⛳️2 Questions for don't miss diagnoses (
@rabihmgeha
)
- Schistocytes?
- Heparin?
⛳️Thrombosis + thrombocytopenia?
- DIC
- HIT
- APLS
- PNH
Framework derived from
@AndreMansoor
's diagnostic buckets!

3
84
305
Compendium of ECG findings concerning for ☠️♥️occlusive MI ♥️☠️ (1/11)

6
105
285
✨ Approach to Infiltrative Diseases! ✨
This framework was inspired by
@Gurpreet2015
's recent Clinical Problem Solving Grand Rounds for
@UCSFDOM
. Many teaching points on this DDx also passed down by the
@CPSolvers
.
First, what are the Infiltrative Diseases?

11
106
286
ILD clues for the internist: here's a 🧵with some quick hits!
Framework by
@DrEricStrong
:
1/12

7
118
281

🩸 Paraprotein Evaluation 🩸
SPEP, SIFE, SFLC, UPEP, UIFE.
What do these abbreviations mean & how does one arrive to the land of paraproteinemias?
Here is a tweetorial for the internist diagnostician, in collaboration with
@cullen_lilley
!

9
96
245
Approach to Altered Mental Status, revisited! Pearls on stroke subtypes via
@AaronLBerkowitz
, Pre- vs. Intra-brain via
@rabihmgeha
.

3
60
236
Everything HLH!
1) Pathophys (uncontrolled macrophages/lymphs.)
2) Diagnostic criteria & Triggers (
@rabihmgeha
)
3) Rx (
@AaronGoodman33
)
4) Other "cytokine storm" etiologies/triggers
References:
1)
2)
3)




6
57
234
🫁🩸 Framework for Pulmonary Disease in Lupus 🩸🫁
1st pass = Infection & Chest well pain
2nd pass = Acute vs. Chronic presentation of respiratory symptom(s)

2
60
235
Awesome to see 24-hr call be eliminated slowly through my
@YaleIMed
residency, now to be completely in the past beginning next year! 👏
@MarkDSiegel1


2
22
227
Peripheral edema + *no* intra-thoracic edema + normal LVEF does not always= isolated R.-sided CHF.
Other major culprit? HFpEF!
Why?
First, ⏫ LVEDP (>15 mmHg) causes pulmonary venous HTN...

2
57
204
DDx of non-cirrhotic hyperammonemia!
1) Heme disorders 🩸🦀
2) Urease-producing infections 🦠
3) Drugs 💊
4) Urea cycle defects, unmasked 🧬
Framework via:


2
68
199
🟤 Approach to Acute Hepatocellular Injury 2.0 🟤
- Was previously missing a Metabolic category, which I added to Toxic category, as these diseases can mimic EtOH-assoc. hepatitis (eg Wilson's)
- Added anti-SLA antibody as 2nd-pass AIH work-up

🟤 Approach to Acute Hepatocellular Injury 🟤
The DDx of ↑ AST & ALT out of proportion to ↑ in cholestatic labs is easy for most.
BUT! I think some can't-miss conditions are frequently left out by early learners.
Here's a diagnostic approach that'll prioritize those causes.
6
95
331
2
71
198
🟡 DDx of AKI 🟡
AKI is a proximal diagnosis requiring a final etiological explanation.
In other words, when encountering AKI, one must ask, "why?"
Here's a one-pager organized by AKI's etiological buckets, which encourage the pursuit of an endpoint diagnosis!

3
39
182
❓ An encapsulated case challenge for your Monday! ❓
A middle-aged human presents to the ICU for management of the following severe metabolic derangements:


11
51
180
💊💩 Typhlitis, an illness script! 💩💊
"Tuphlon" = Greek for 'cecum or blind gut'
-itis = Inflammation!
Also called Neutropenic enterocolitis!

2
47
169




🪟 Pulmonary Alveolar Proteinosis (PAP) 🪟
- Rare cause of insidious-onset dyspnea on exertion
- On DDx of Crazy Paving on chest CT
- Due to 👇 production/clearance of surfactant



4
50
154
This was an ECG I saved from a woman w/ metastatic renal cell carcinoma who had acute dyspnea, tachycardia, & hypoxemia while in the hospital.
What classic ECG findings are show here & what test would you send next?
The bottom strip was taken 24hrs prior to the top strip!

8
36
155
🧠 An updated unified approach to Altered Mental Status! 🧠 Inspiration from
@CPSolvers
iterations of MIST 1.0 👉 2.0 👉 "MIST negative"
@rabihmgeha
@DxRxEdu
@AaronLBerkowitz
@MariaMjaleman

4
33
154
🟤 Hepatomegaly Schema 3.0 🟤
- Schistosomiasis = worldwide most common
- (N)AFLD = U.S. most common
- Split DDx into tender vs. non-tender (exceptions always possible)
- Massive hepatomegaly? → R. heart failure, mets., hepatosplenic T-cell lymphoma, cystic disease

5
38
132
Exercise-induced urticaria!
Interesting case report & review by undergrad friend!
.

1
20
123
VEXAS Syndrome
🧬 Somatic mutations in UBA1, enzyme starting ubiquitylation
👇
🧬 Rx-refractory inflammatory disease, cytopenias (dysplastic marrow w/ precursor vacuoles), neutrophilic cutaneous & lung inflammation, chondritis ("RP-like"), & vasculitis

4
34
125
🔵 Approach to Rituximab Adverse Effects 🔵
@MithuRheum
, a product of being on rheum consults next 2 weeks!
What did I miss?

8
32
123
Teaching
@ClementLeeMD
's approach to Acute Hypoxemia! 🫁
No better way to get through the major DDx with ease. Students always love this one.
All while on the Klatskin service with Dr. Schilsky (
@Dr_Aly_Fox
)


1/14
Rapid Response Series,
#3
: Hypoxia
How many times on rounds have you been asked, “What are the 5 causes of hypoxemia”? 🤔
#MedTwitter
#TipsForNewDocs
7
89
265
3
23
120
How can med schools better reconcile the pre-clinical teaching of pathology with the teaching of practical clinical knowledge; among that, schematic diagnostic thinking?
@AndreMansoor

3
10
119

2 early repolarization variants (funky ST-T segments) to learn & save!
♥️ Benign early repolarization
♥️ Benign T-wave inversion
1/


1
33
107
🧠Approach to Altered Mental Status🧠
Re-formatted for readability + highlighted metabolic labs/work-up that can be acquired in the undifferentiated patient!

Approach to Altered Mental Status, revisited! Pearls on stroke subtypes via
@AaronLBerkowitz
, Pre- vs. Intra-brain via
@rabihmgeha
.
3
60
236
0
27
109
An approach to hepatomegaly! Maybe helpful for those feeling a little extra distended post-Thanksgiving. Clues to diagnosis are written in (parentheses).
@ebtapper
, would love your thoughts! Adapted from:

1
25
108
🟡 Monoclonal Gammopathies of Renal Significance (MGRS)! 🟡
How should we organize this long list of Paraprotein-mediated, kidney-damaging diseases?
Heme/onc aficionado
@MatthewHoMD
& I teamed up to simplify things for the diagnostician.
Let's re-do MGRS.

3
37
109

Excited to once again release an updated version of my Anki deck for ICU preparation! This deck is best suited for M3/4s & interns new to the ICU: below is Version 6 of this ICU deck, which I started working on early in the pandemic last year...

3
16
105
🟢 Non-cirrhotic Hyperammonemia in Adults 🟢
- Hematalogic & Vascular (liquid cancers + wonky portal venous vasculature) 🩸
- Urease-producing bacteria (symptoms if urinary retention + elderly) 🦠
- Unmasked Urea cycle Defects (namely, OTC deficiency + stress) 🧬
- Drugs 💊

4
29
100
Really nice new website & podcast covering core inpatient medicine topics: Point of Care Medicine 🩺
Incoming interns should definitely check this out, as there are helpful templates for new admits, workup, etc. specific to particular chief concerns!

2
25
101
❗️Rapid Diagnosis Challenge❗️
A middle-aged human with "COPD" (no PFTs on file, on chronic 2L), HFpEF, & morbid obesity presents w/ subacute DOE → resting dyspnea & worse hypoxemia:
🫁 SpO2 86% on 6L
❤️ Other VS show: no fever, HR 100s, 110/70s

7
12
98
Transient (<30 min) hypoxemia in the hospitalized patient 🫁🩸:
- Flash pulm edema (2/2 exertion vs. ischemia vs. tachyarrhythmia)
- Orthodeoxia (2/2 Intrapulmonary vs. Intracardiac shunt)
- Mucous plug
- ??? What else ???
@nsrosenberg
19
16
95
❓ An encapsulated case challenge for your day! ❓
An elderly human presents with subacute nausea/vomiting, abd pain, dyspnea on exertion, & leg swelling
Their history is remarkable for adult-onset Still's disease currently off immunosuppresives due to recent severe infections

1
31
89
Cardiorenal AKI pearls via
@thecurbsiders
:
⚪️ Increased SCr during CHF admission once shown to be assoc. w/ improved outcomes (“permissive hypercreatinemia”)
⚪️ Increased SCr through diuresis does NOT necessarily = kidney injury

2
22
94
Here is a thread for the new interns on approaches to common electrolyte derangements: handy reference for both IRL medicine & boards medicine! 🖋️
(Vast majority of the info comes from
@DrEricStrong
's video series.)
Hypokalemia 🍌

1
25
91
😊Obesity Hypoventilation Syndrome😊
Here is an illness script that must be shared over & over again!!
Today we are sharing because I recently saw "OHS exacerbation" used to describe an acutely dyspneic patient with class 3 obesity, acute hypercapnia, & who was admitted with a
3
27
94
@Janetbirdope
Something on this DDx 🙂 (I hope!)
☠️ Approach to Ischemic Limb Syndromes ☠️
You're in the ICU examining a patient & find a patient with purple discoloration of an extremity concerning for limb ischemia
But the patient *has* distal pulses!
What's going on? 🧐
Take a journey with me &
@OmarosisFugax
!
7
132
325
1
16
89
Another rare one, courtesy of
@KirtanPatolia
- always learning from you!
“When APLS isn’t APLS.” 👉 Sneddon Syndrome

2
19
87
First round winners of Connecticut
@ACPinternists
’ Doctor’s Dilemma competition! 🏆
Lucky to work with such awesome co-residents…
@YaleIM_Chiefs
@YaleIMed
@marywhite_md
@BannaSoumya
@MDVictorJimenez

7
6
87

🩸Atypical, Breakthrough, & Multiple Episodes of Thromboembolism in Malignancy🩸
DDx:
- Nonbacterial thrombotic "marantic" endocarditis (particularly, mucin-secreting adenocarcinomas)
- Trousseau phenomenon (migratory thrombophlebitis)
- Chronic DIC
- Acquired APLS


1
21
80

❤️🔥 Myocarditis: the Diagnostic Journey ❤️🔥
It's been a while,
#MedTwitter
!
Today,
@Gurleen_Kaur96
,
@Mark_Heslin
, & I bring you our diagnostic approach to myocarditis.
First we'll give a lay of the HFrEF land; then, we'll cover presenting features & Endpoint DDx.
Onward!

2
30
83
EPIC HACK FOR INTERNS (inspired by
@Karan__Jani
)! One way to ⏫ lab review efficiency is to make .dotphrases for labs you commonly trend! (Think: platelets in heme patients, creatinine in ICU patients.) Here's a .dotphrase I made for a trend of 5 most recent plt counts! 1/5

5
9
81
How to Teach Dx Reasoning 🕵️♀️
🕵️♀️ 1) Read Penner, Shipley, & Minter's "Reasoning on Rounds" article:
🕵️♀️ 2) Incorporate
@ArcieriMichael
's cognitive forcing strategies into the development of problem representations & prioritized DDx development


Internal medicine clerkship is where medical students (regardless of their interest) should learn the art of diagnostic reasoning. But we have very little training in how to teach it. Here is my approach: 👨🏫
#MedTwitter
1. The Rule of 3’s
2. The 3 C’s
3. 20-50-80
36
679
3K
0
26
79


Then & now 😄
@AndreMansoor
, the Dx community is forever grateful for your updating this legendary book!
Also, the colors are awesome!


3
4
76
✨ Approach to Infiltrative Diseases 2.0 ✨
- After reading original 🧵 linked in this specific tweet, see new 🧵 below for beautified one-pager & illness scripts!

✨ Approach to Infiltrative Diseases! ✨
This framework was inspired by
@Gurpreet2015
's recent Clinical Problem Solving Grand Rounds for
@UCSFDOM
. Many teaching points on this DDx also passed down by the
@CPSolvers
.
First, what are the Infiltrative Diseases?
11
106
286
2
26
70
❗ Cardiology Dx Challenge ❗
An elderly human with multiple cardiovascular risk factors presents after awakening on the floor unsure how they got there. The night prior, they had new vague abdominal discomfort & b/l shoulder discomfort.
The admission & baseline ECGs are below:


8
13
74
A library of ECG patterns concerning for occlusive MI to review during your holiday travels! 🎄✈️
Remember, ~25-30% of NSTEMIs are found to have complete coronary occlusion on cath: ↑ short-term mortality (RR 1.67) & MACE (RR 1.41)!
🔗
👇👇👇

3
22
74
Excited to share my 1st case report: Legionella & S. aureus co-infections in a patient with SARS-CoV-2!
Sharing this case & its reminder of important clinical lessons not possible w/o
@YaleIDFellows
's Eric Elliot & Anne Spichler-Moffarah, &
@YaleIM_Chiefs
's Peter Wang.

5
15
69


A story of a patient of mine with a rare cause of dysphagia.
@LisaSandersmd
, thank you for sharing his story!

7
10
69
🫁 Approach to Interlobular Septal Thickening 🫁
Attempted to simplify this fun DDx in this living
@GlassHealthHQ
page
👇

0
26
69
💭 Tips 💭:
1) Save & keep your resources organized!
I use
@msonenote
&
@GlassHealthHQ
&
@appleicloud
for collecting/organizing notes that ultimately get sent to my learners:



6
7
69
Practice your hemolysis journey here!
👇
Framework by
@AndreMansoor


CASE STUDY
1/11
74 yo F presents with CBC shown in graphic below. You will note she has macrocytic anemia, which has a wide differential diagnosis (also shown in graphic).

7
94
359
0
21
67
Great hemoptysis case on
@CPSolvers
this AM prompting coags investigation for the first time in a while.
@DrEricStrong
's coags approach &
@NikitaSonaliyaD
/
@Gurleen_Kaur96
's hemoptysis approach below! Thanks all!



5
16
67
Triad of CHF review for the return to wards:
@AndreMansoor
's diagnostic approach,
@cardionerds
' podcast on GDMT, & NYP's CHF guidelines

1
13
67
I consider reading
@AndreMansoor
's Frameworks for Internal Medicine (cover to cover) during my M3-4 years my personal initiation into the world of Dx 🌎
Anyone interested in mastering medicine should be stoked about Ed. 2!

10/10
Dysphagia is one of 8 new chapters in Frameworks for Internal Medicine 2nd Edition, set to be released this summer.

10
20
256
2
4
66
Always nice to be able to pull up one of
@AndreMansoor
’s frameworks when I’m rusty; thanks
@CPSolvers
for this morning’s great case!

2
10
61

Rising
#MedTwitter
#MedX
interns, here are my favorite approaches for acute inpatient medicine issues! 🚨
1) Hypoxemia, by
@ClementLeeMD
🫁
Ditch the alveolar gas equation (sorry
@PulmPEEPs
) & use this practical approach.
1/14
Rapid Response Series,
#3
: Hypoxia
How many times on rounds have you been asked, “What are the 5 causes of hypoxemia”? 🤔
#MedTwitter
#TipsForNewDocs
7
89
265
2
15
63
First time senior-ing was an absolute pleasure with star
@YaleIM_Chiefs
PGY-1
@NarulaSukrit
!
Also can’t forget our great med student Robert Tseng!

2
2
61
🩸Portal biliopathy🩸:
*Chronic* portal vein thrombus
👇
Venous collaterals ("cavernous transformation of portal vein")
👇
Biliary obstruction!


1
11
60
Thrilled to open 2024 with a case just published in
@BrownJHM
: "Pulmonary Infarction Due to Direct-acting Oral Anticoagulant Malabsorption" 🥂
We hope this 📄 will be considered a "must-read" for clinicians who diagnose & treat PEs!

2
12
59
@BrownHospMed
@Radiopaedia
Melioidosis – one of the non-filamentous chronic pneumonia diseases.
☂️ Burkholderia pseudomallei inhaled in ST Asia
☂️ Imaging: miliary nodules → cavitary lung disease
☂️ Presentation: fever → hemoptysis
☂️ Risk factors: DM, CKD, EtOH

2
4
60

13
0
57
Approach to Polyneuropathy 🧠
Re-sharing my old 🧵along with a
@GlassHealthHQ
page with the notes I reference every time I see this chief concern!
👇

1
14
57
Today in the Step Down Unit I saw:
- Type B Lactate of 8 (ETOH intox., thiamine deficiency)
- Native hemolysis of cirrhosis (no spur cells)
- Int.-risk PE p/w dyspnea-on-chewing
- New L/R-sided infective endocarditis
- ?Pulmonary tumor emboli (
@Heard_that_alex
)
IM is awesome!
2
1
56