

Thomas Eliot Lew
@thomaseliotlew
Followers
303
Following
1K
Statuses
232
Doc from Melbourne, Australia. Treats patients with blood cancers and researches new therapies. Loves family, immersive theatre and running.
Melbourne, Australia
Joined June 2020
10ys of insights from treating pts with #CLL after venetoclax at @PeterMacCC & @TheRMH summarized in this latest review. Our approach to sequencing novel agents, venetoclax re-Rx and cellular therapies. Privilege to work with giants Prof Tam & Seymour

3
4
33
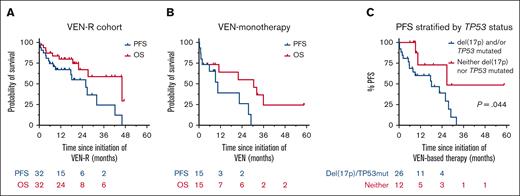
Great to see this in print! VenR is active in BTKi (and mostly chemo) exposed CLL, but most pts will develop PD during or shortly after 2y on VEN Time limited Rx a rarity in this context Appears comparable to PIRTO Lots of room for improvement here @Eddie_Cliff @victorshiyulin

Venetoclax-rituximab is active in patients with BTKi-exposed CLL, but durable treatment-free remissions are uncommon #researchletter #lymphoidneoplasia
1
2
9
High calibre company and a fun night indeed!


1
0
2
Nice data! We’ve observed similar results in our Australian cohort. VenR achieved responses in cBTKi-exp, but a mPFS of 26m. Worse if p53 abn. Rx free remission with VenR post cBTKi is uncommon, and outcomes are modest Very different from chemo only exp pts as in MURANO

Dr. Samples (@LauraSamplesMD) will present her second poster today. Outcome of pts with #CLL who received venetoclax after failure of cBTKi. @fredhutch data. A very relevant clinical question. #ASH23
0
0
1


Ribrag #ASH23 MCL >60 or auto ineligible 1L Randomisation 1: RCHOP v RCHOP/RHAD – no PFS difference Randomisation 2: Len-R v R as maintenance – PFS better, no OS difference R2 definitely more toxic, infections & 2nd malignancies Seems clear to me – don’t add LEN to maintenance!




0
0
1
Going to be wild! Can’t wait #ASH23

Looking forward to presenting our recent work from @TheDawsonLab at #ASH23 this afternoon! We use SPLINTR linage tracing to understand the clonal and transcriptional dynamics of the rare clones that contribute to B-ALL relapse after CAR-T
0
0
1
Kumar #ASH23 – impressive work BOVen (ZANU, Obin, VEN) for TP53mut MCL 1L N=25 Tox profile looks good - G3+ neutropenia 12%, G1 diarrhea common ORR 96% CRR 88% 2yPFS 72% 2yOS Frequent uMRD The best outcomes ever achieved in this high risk group




0
2
4
And nice MRD data from Andy Rawstron Using I+V, BM uMRD-4 is confidently predicted by: PB uMRD -5 once PB uMRD-4 on two recordings 6 months apart #ASH23
Hillmen #ASH23 FCR v MRD I+V 1L fit CLL (Rx 2x time to uMRD) I+V: Higher BM uMRD (62% v 40%) PFS & OS signif better (but driven by IGHVunmut) More tMN & TRM in FCR Lots of Qs: - Who really needs 1L doublet? IMO - not all - Fixed dur vs MRD driven? - Will re-Rx work? IMO - yes



0
1
0
Hillmen #ASH23 FCR v MRD I+V 1L fit CLL (Rx 2x time to uMRD) I+V: Higher BM uMRD (62% v 40%) PFS & OS signif better (but driven by IGHVunmut) More tMN & TRM in FCR Lots of Qs: - Who really needs 1L doublet? IMO - not all - Fixed dur vs MRD driven? - Will re-Rx work? IMO - yes
0
2
4
High (and deserved) praise for @drchynchua!



1
1
6
Too kind Eddie! A terrific session on novel targets in blood cancers
Congrats to the fab @thomaseliotlew for clever translational work & an articulate oral presentation on the role of the mitochondrial E3 ligase MARCH5 and how its depletion leads to synthetic lethality to venetoclax #ASH23

0
0
2
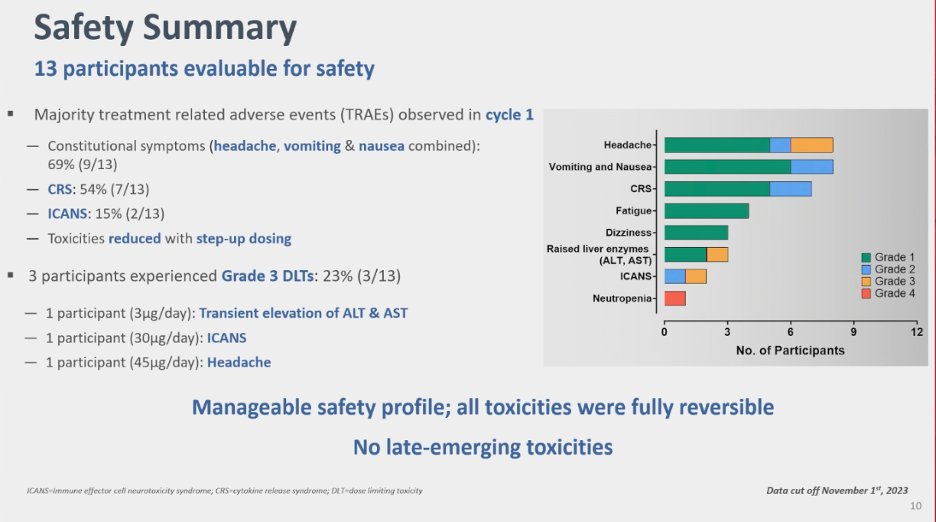
Jasani #ASH23 P1 trial: ROR1-CD3 bispecific +/- IBR Short t1/2, admin via CADD 12 response eval pts Unclear how high risk they really were ORR 58% MRD-4 in 3 CLL/PET CMR 1 MCL CRS 54%, ICAN 15% (1 G3) Limited data, admin difficult, CRS & ICANS Still - deep remissions w/o BCL2i!



1
2
5
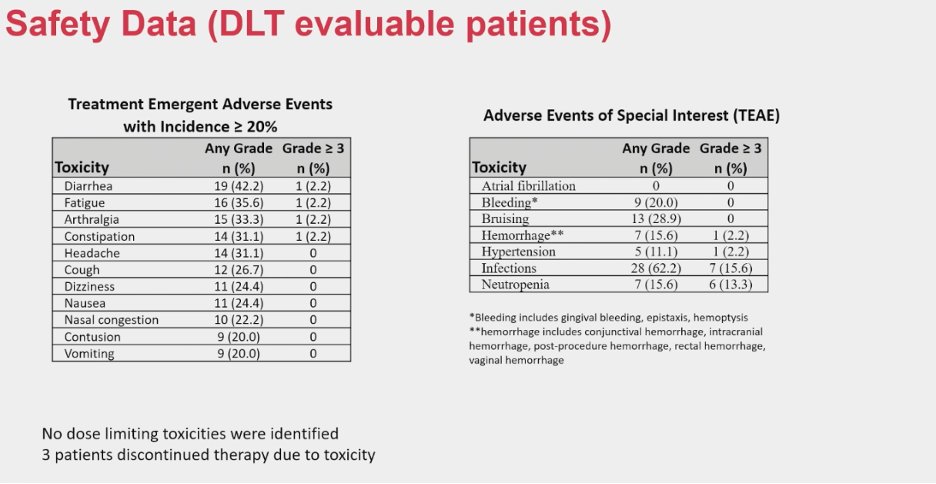
Woyach #ASH23 P1 trial: LP-168, dual cov & non-cov BTKi Binds C481S & gatekeeper mut BTK N=37 CLL (21 C481S, 9 T474) Bleeding/bruising in 15-30%, all <G3 Infections in 62%, no AF ORR ~70% at ≥200mg/d (no CR), sim if T474mut RP2D 200-300mg/daily No data for L528W… one to watch!



0
0
3
Feels like there is a subset of patients that benefit from the CPI+BTKi approach, but how do we identify them or, ideally, build on the regimen to do better? OS surprisingly good in this cohort despite modest efficacy... makes me wonder if this is a special/selected group

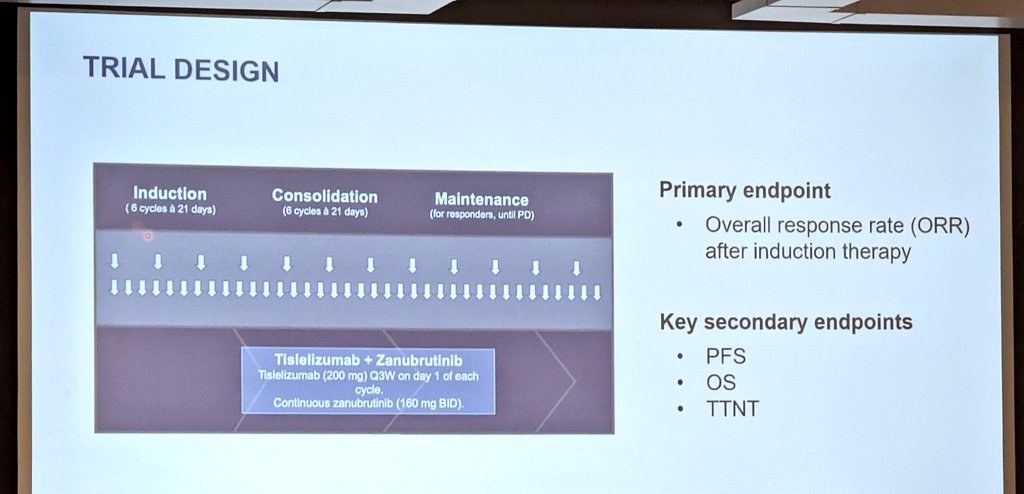
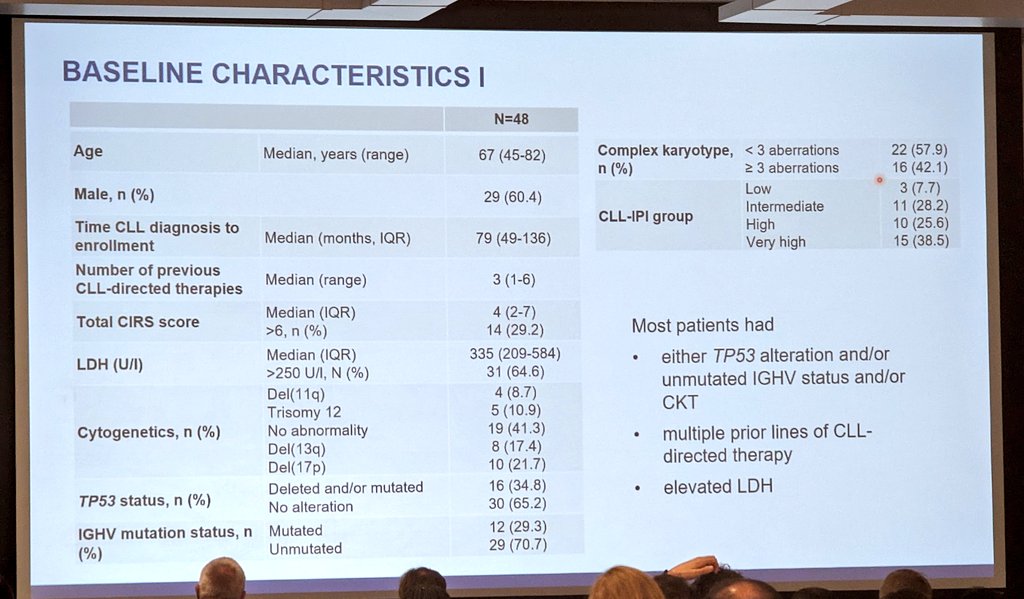
Tislelizumab+zanu in Richter's #ASH23: - 48 pts, 80% untreated for RT, 35% TP53mut - 7 possible irAEs (mostly ⬆️LFTs), 3 Gr5 infx - ORR 58% (CR 19%), mDOR NR - mPFS 10 mos (only 7 mos in ITT), mOS NR! Bridging to allo option? PFS still not great. #lymsm #leusm


0
0
2
Al-Sawaf #ASH23 P2 trial Tislelizumab + ZANU for ���2L RT N=48 ORR/CRR 58.3% / 18.8% mPFS 10m/1yOS 75% Well tolerated Could bridge to allo Planned protocol amendment to add sonrotoclax coming Overall modest, but durable responses for some Now out in Nat Med! Baby steps for RT...




0
0
1
Pretty impressive, particularly for BTKi/VEN exposed pts, for whom outcomes with 2nd target agent usually achieve mPFS ~24m and true time limited Rx uncommon Is the best place for doublets/triplets as next Rx after 1st targeted agent? May be better than doing this for everyone..
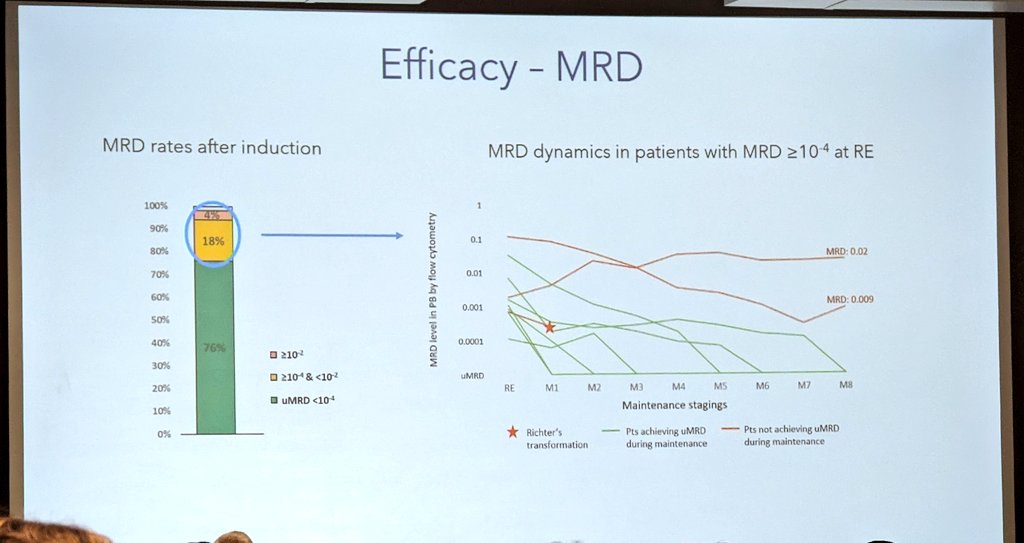
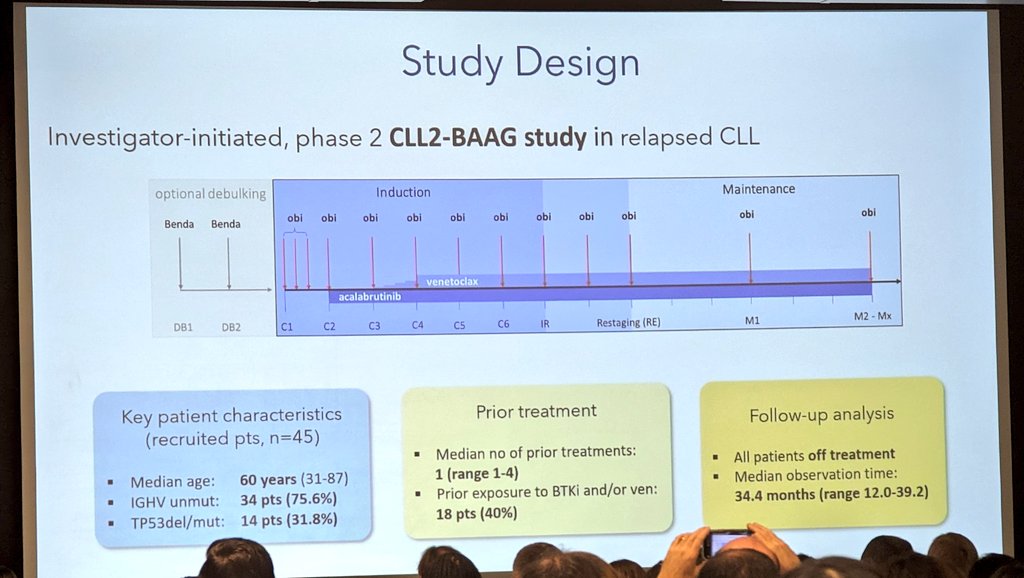
MRD-adapted ven+obi+acala in R/R CLL #ASH23: - 45 pts, median tx duration 14.7 mos - 76% uMRD, med time to uMRD ~5 mos - 94% uMRD even if prior BTK/ven Interesting time-limited option; optimal sequencing with 1L? #lymsm #leusm


0
1
6
Moskowitz #ASH23 Ruxo for RR T-LGL Seems highly effective in pts with STAT3 mut Correlative data suggest STAT3mut T cells drive ^ JAK/STAT in the myeloid compartment, and ruxo is acting here to improve disease. V interesting! Could be a nice option for some tricky cases…




0
0
2
Nice (and huge) dataset Matches a few other series in this space Incorporation of CPI prior to auto for RR cHL seems to improve outcomes #ASH23 #lymsm
PD1 before ASCT retrospective #ASH23: - 981 pts (!!), 20% PD1+/-BV preASCT - superior PFS if got PD1 (vs BV or chemo alone), also in MV model - no difference in OS Huge cohort and I try to give CPI to all R/R cHL prior to ASCT. #lymsm




0
1
3
Rutherford #ASH23 Pts ≥60 in S1826 (AVD + BV v Nivo in adv HL) Nivo: More neutropenia, hypoT & rash, less sepsis & neuropathy Lower NRM 4% v 14% Big EFS improvement (1y 93% v 64%) 1y OS 95% vs 83%, p =0.091 Slam dunk – more effective, better tolerated, new SoC for elderly cHL!




0
2
6
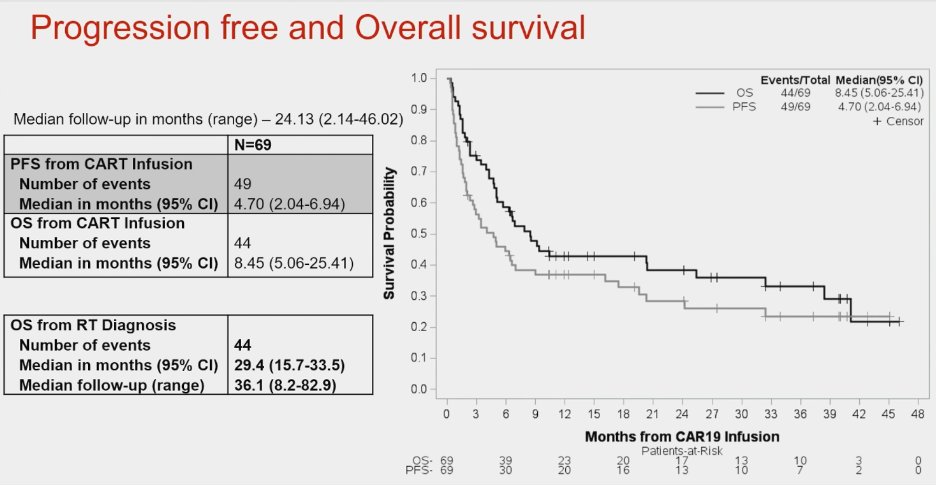
Kittai et al #ASH23 RWE for CD19 CART for RT (USA & Aus) N=69, genetically adverse, 84% VENorBTKi use for RT Mostly axi-cel 65%, 45% with concur BTKi mFU 24m, ?plateau around 25-30% PR - no durability TRM 27% - toxic!! Likely lots of unmeasured selection for pts to get here



0
1
3