

Lee Zhao
@lee_c_zhao
Followers
5K
Following
4K
Statuses
1K
Reconstructive Urologist, NYU Langone Health, views are my own https://t.co/LDinyQ04SU
New York
Joined March 2011
@youness94856331 @YouTube yes, make a small hole, but don’t empty the hydrocele completely to help identify the correct layers.
0
0
1
I prefer the retro approach for redo pyeloplasty: avoids vasculature and direct view of UPJ. Redo Y-V plasty via retroperitoneal approach, SP robot via @YouTube
0
1
24
@ZhinaSadeghi @YouTube Yes, this approach is my preferred technique for redo pyeloplasty also. I will post a video.
0
0
2
@gkhvadagiani @YouTube This technique pulls the UPJ away from the crossing vessel. Don't have to translocate the ureter to the other side--I have done that in the past, and it seems like the vessel will obstruct from the other side.
1
0
0
@amorgado4 @YouTube find the patient’s left corpora, dissect towards surgeon’s left (medial) to find dorsum of urethra. with urethra rotated to patient’s right, the urethrotomy will be exposed to the surgeon’s right hand for forehand suturing of the graft.
1
0
0
@basalmind @YouTube The Vision Pro is heavy, but can be worn for 50 minutes without pain. One drawback is that there no magnification with it, so have to be able to see the tissue without loupes. For surgery requiring loupes, I am still working on a good recording solution.
1
0
2
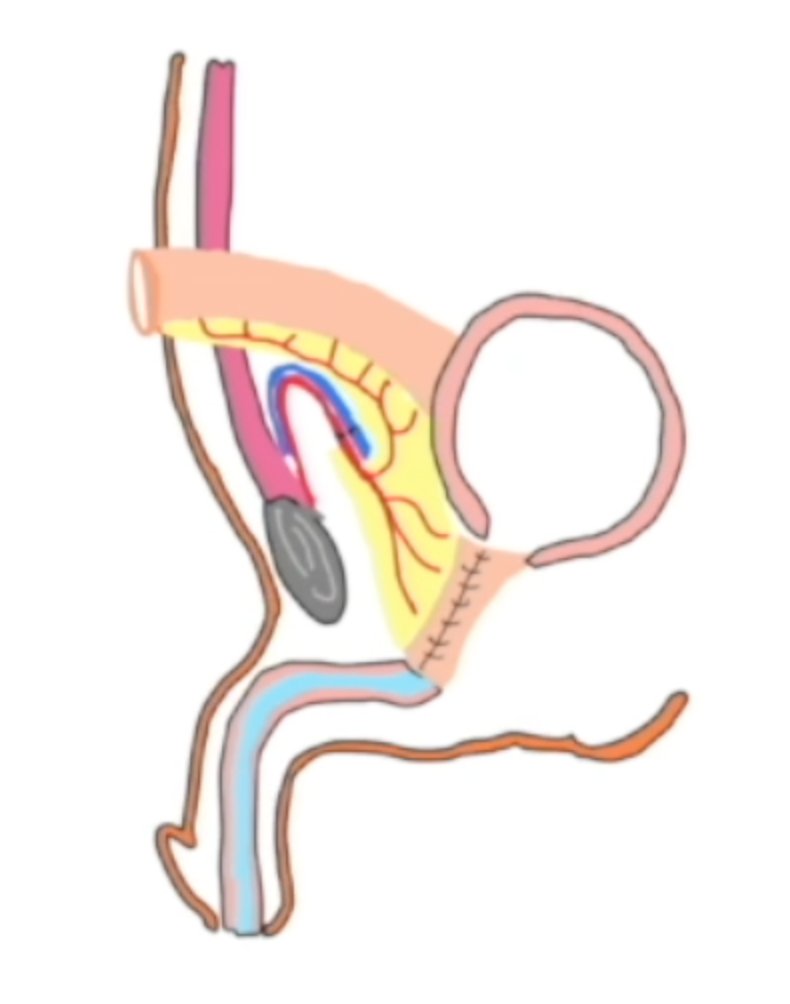
It is an incredible honor to present at best case #ASRM2025 @asrm_micro our robotic ileal free flap for end-stage pelvic radiation injury. After searching for years, Jamie Levine and I @nyulangone have developed a promising technique of free tissue transfer. More info to come!

2
0
43
@amorgado4 @SPuro88 @GiorgioI_Russo @drMarcoFalcone1 @ManfrediCeleste @simo_cilio @drserefoglu @donwglee @allen_morey @UTSWUrology I would start perineal to see what the tissue looks like. If dissection is so hard that there is risk of urethral injury, then switch to transcorporal placement.
0
0
4
@amorgado4 @SPuro88 @GiorgioI_Russo @drMarcoFalcone1 @ManfrediCeleste @simo_cilio @drserefoglu @donwglee The major issues with AUS erosions is how to set up the urethra for the next AUS surgery. I think a urine leak incr risk of stricture and periurethral fibrosis, so I use 2-0 PDS to do an “in situ” urethroplasty as I learned from @allen_morey @UTSWUrology fellowship.
2
0
2
One "killer app" for the SP robot is retroperitoneal access via from a supine position via an incision 2/3 betw umbilicus and ASIS. This video shows the Supine Anterior Retroperitoneal Access on the right. via @YouTube
0
1
26
This is a great technique and even better description. It is hard to see the upper pole in the supine anterior retroperitoneal access, and the gauze is a great way to climb to the upper pole.

Upper pole exposure during SP kidney surgery #1: “Climbing with gauze.” Have you ever watched a mountain climber working their way up a steep face. They inchworm up the face setting safety points into the rock as they go. They take the larger face in smaller segments and secure their gains as they go. If something unexpected happens, they don’t lose all their progress and have to start over. Climbing to the extreme upper pole from low anterior access can sometimes feel like climbing a rock face. You can mimic the climber by carrying a gauze with you as you climb the diaphragm or underside of the peritoneum to reach the extreme upper pole and take down attachments. As shown in this video, move forward incrementally then set the gauze to hold your exposure gains before moving forward again. Inchworm your way up and save yourself frustration when the tumor is large and adherent to adjacent structures.
0
1
21
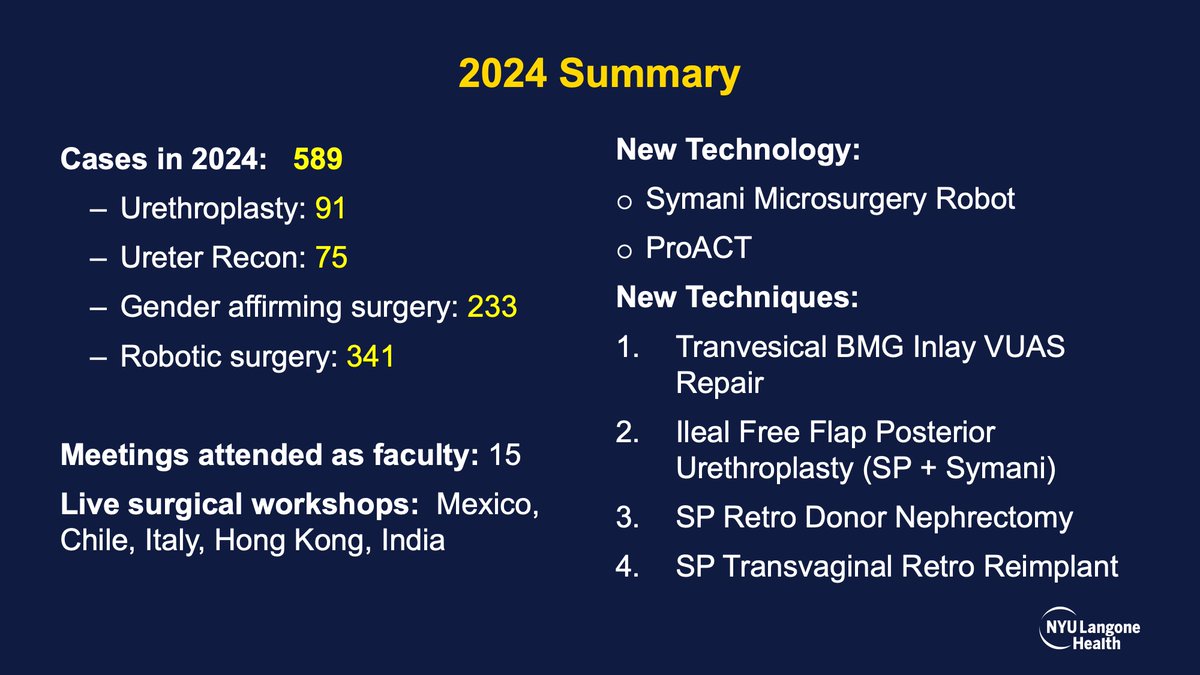
Annual review: 2024 was productive. ~600 cases, ⬇️urethroplasty (⬆️Optilume),⬆️ureter recon, ⬆️robot📈innovation. Lucky to be at the right place @nyulangone, privileged to train residents, fellows, colleagues, & grateful for the trust patients have placed in me. Happy New Year!
8
3
132
Rectourethral fistulae are challenging. Many series that report good outcomes exclude patients with "large" or "unreconstructable" fistulae. I offer repair to most patients using robotic abdominal approach. Full length case from CILR 2024 via @YouTube
0
6
49
RT @ysaralee: Sharing our article on single-port RA lap ureterocalicostomy. Thank you to the team @NYUUrology for the opportunity to contri…
0
8
0
>11 years ago, @mdstifelman and I performed 1st robotic buccal mucosa graft ureteroplasty (video) @nyulangone. @md_eun joined us after learning of the technique @Endo_Society mtg to form #CORRUS. Here is our decade long follow up: n=163, 92% success.
0
11
92
@RoboDocX @CanesDavid @mdstifelman @md_eun @wiegand_luke Yes agree. definitely some patients with patent ureter and pain after recon. Autotransplant seem to help. The question is whether the fix is the shorter ureter or denervation of the kidney via transection of the vasculature.
1
0
4