

Jason Scott Hauptman MD PhD
@jshauptman
Followers
1K
Following
140
Statuses
460
Husband | Dad of 3 | chief of neurosurgery @phxchildrens | professor @uarizona @barrowneuro | tumor-epilepsy-stereotactic-functional neurosurgery in children
Phoenix, AZ
Joined May 2010
Multiple. But I don’t think the issue with poor outcomes in MTS in children is really due to inadequate temporal disconnection. I think it’s the high incidence of dual pathology that leads to LITT being insufficient. I’m less enthusiastic to do up front LITT for temporal pathology in children in general.
0
0
2
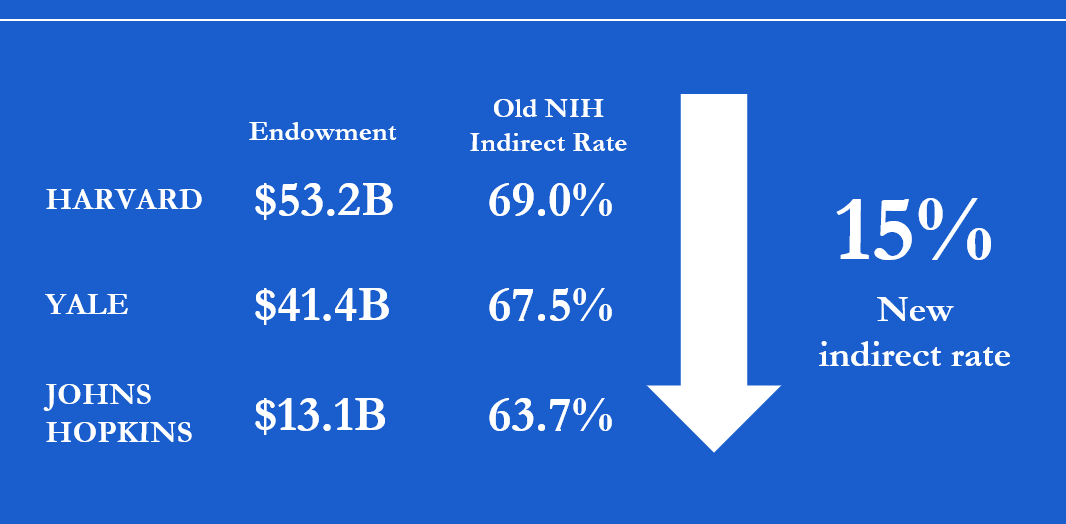
Whoa strap in this is going to be a big deal

Last year, $9B of the $35B that the National Institutes of Health (NIH) granted for research was used for administrative overhead, what is known as “indirect costs.” Today, NIH lowered the maximum indirect cost rate research institutions can charge the government to 15%, above what many major foundations allow and much lower than the 60%+ that some institutions charge the government today. This change will save more than $4B a year effective immediately.
0
0
1
7F with a recurrent posterior fossa solid JPA in the left cerebellar hemisphere. I think this is a great application of LITT. Certainly this could be resected through a revision craniotomy. But LITT is a very reasonable option. Single 10mm. No hair shave, small incision, home the next day! #neuro #neurotwitter #braintumor #neurosurgery @PhxChildrens @BarrowNeuro

0
6
20
12F with LGS and atonic-predominant medically intractable epilepsy. Offered LITT callosotomy. Our preference is to do anterior 80% first as we’ve found it to lessen the disconnection symptoms post op. Three 10mm, one for rostrum and two for the body. If needed can always go back and do the splenium later. #neuro #epilepsy #neurosurgery #neurology #neurotwitter @PhxChildrens @BarrowNeuro



0
0
0
Revision ATL in a teenage girl with a previous medial temporal LITT that failed. I find these cases always a little tricky, as many times the temporal horn is scarred and the choroid is stuck to the hippocampus. The ablated tissue is always quite firm and adherent to the pia. That on top of the high failure rates of medial temporal LITT in children makes me wonder about LITT in these cases. Opinions? @PhxChildrens @BarrowNeuro @barrowpch

0
1
22
@AlyssaJonykiene @TheASPN @PedsSection @CNS_Update @AANSNeuro @AANSNeurosurg @wearecbtn @NSTumorSection I agree subfrontal felt like the right choice. I knew it would limit how far back and high i could get. You always wish you could get more but I didn’t want to push the visibility.
0
0
1
@MaxKrucoff_MD @TheASPN @PedsSection @CNS_Update @AANSNeuro @AANSNeurosurg @wearecbtn @NSTumorSection Very kind words from an excellent tumor surgeon in your own right. Thank you. This was a tough one for sure.
0
0
0
@AuthentiquEtre @TheASPN @PedsSection @CNS_Update @AANSNeuro @AANSNeurosurg @wearecbtn @NSTumorSection Yeah there may need to be a second approach from the top
0
0
1
@rweichselbaum @TheASPN @PedsSection @CNS_Update @AANSNeuro @AANSNeurosurg @wearecbtn @NSTumorSection I agree xrt has to be in the future but only 2 years old. Also agree need to think about toci/avastin if no more surgery.
0
0
1
@palmasopa @TheASPN @PedsSection @CNS_Update @AANSNeuro @AANSNeurosurg @wearecbtn @NSTumorSection Yep. Papillary exceedingly rare in children. But this was not positive for the fusion.
0
0
2
Bragging about my amazing partners and speaking on hemispherectomy in infants @TheASPN @BarrowNeuro @PhxChildrens @barrowpch

0
0
6
Our experience using the new Inomed frame with @zimmerbiomet Rosa robot. As far as we know this may be one of the first applications in a pediatric patient in the US. First impressions - shaves off time having to place bone fiducials (our standard workflow), less incisions, excellent accuracy. Integrated fiducials, low profile. Great advancement! @PhxChildrens @barrowpch @BarrowNeuro




2
1
19
LITT can be great for low grade glioma. This was a child who had a local recurrence of a JPA in the left occipital region with a coincident cyst that was encroaching on the occipital horn. We placed one catheter in the tumor and then a needle in the cyst, aspirated, and then ablated. Home the next day. @PhxChildrens @barrowpch @BarrowNeuro




1
1
24
RT @JamesRutka: This just out! My colleague Peter Dirks and his lab published on the origins of Glioblastoma from neural precursor cells i…
0
27
0
@Jpb1007Jeffrey @TheASPN @PedsSection @CNS_Update @AANSNeuro @epilepsysociety @PESAlliance @CureEpilepsy @epilepsyaction @neurosurgery @TheJNS In your expert hands - the same!
0
0
1
Hi Jeff this is a great question and i think you and I think exactly the same way- the RNS was done a few years before I met him. My guess is concern over proximity to eloquent cortex and the need to get down into the fissure to hug a bunch of those M3/M4s- but as you alluded to the tissue that is the problem is not functional tissue. I also think we need to make sure with neuromodulation that we don’t blur the line between cure and palliation - which I see happening more.
0
0
3
@Dr_JP_Parker @TheASPN @PedsSection @CNS_Update @AANSNeuro @epilepsysociety @PESAlliance @CureEpilepsy @epilepsyaction @neurosurgery @TheJNS Broad region of spiking essentially across the entirety of encephalomalacia. Interestingly no muscle activation to stim in putative motor.
0
0
0