

Cliff Reid
@cliffreid
Followers
44K
Following
20K
Media
2K
Statuses
14K
EM/ICM/PHEM doc. LOVE learning + teaching. I work in the sky above Sydney, have the attention span of a bullet, + often have days that are like cartoons #FOAMed
https://cliffreid.substack.com
Joined March 2009
I showed a resident how to diagnose a pneumothoraces. She asked 'don't you mean a pneumothorax?'. I replied 'it's pleural'.
206
889
9K
Someone left a stethoscope on the orthopaedic surgeon's desk
271
2K
16K
A patient with a rare condition was brought in to our ED last night - the first one our senior nurse has seen in her forty year career. It was a gunshot wound.
177
603
4K
If anyone knows Kirsty the internal medicine trainee/recent geriatrics clinical fellow from Edinburgh who recently managed an in-flight emergency from Sydney to Hong Kong please tell her she’s awesome & pass on my thanks & Twitter contact so I can give her patient follow up info.
18
678
3K
Just a reminder to all nurses and doctors everywhere that placing a hypotensive patient in a head down position isn’t good for their airway, their breathing, their intracranial pressure (and hence their cerebral perfusion) and doesn’t usually help their blood pressure

67
433
3K
I had multiple attempts to insert the arterial line in the correct vessel but all my efforts were in vein.
56
167
2K
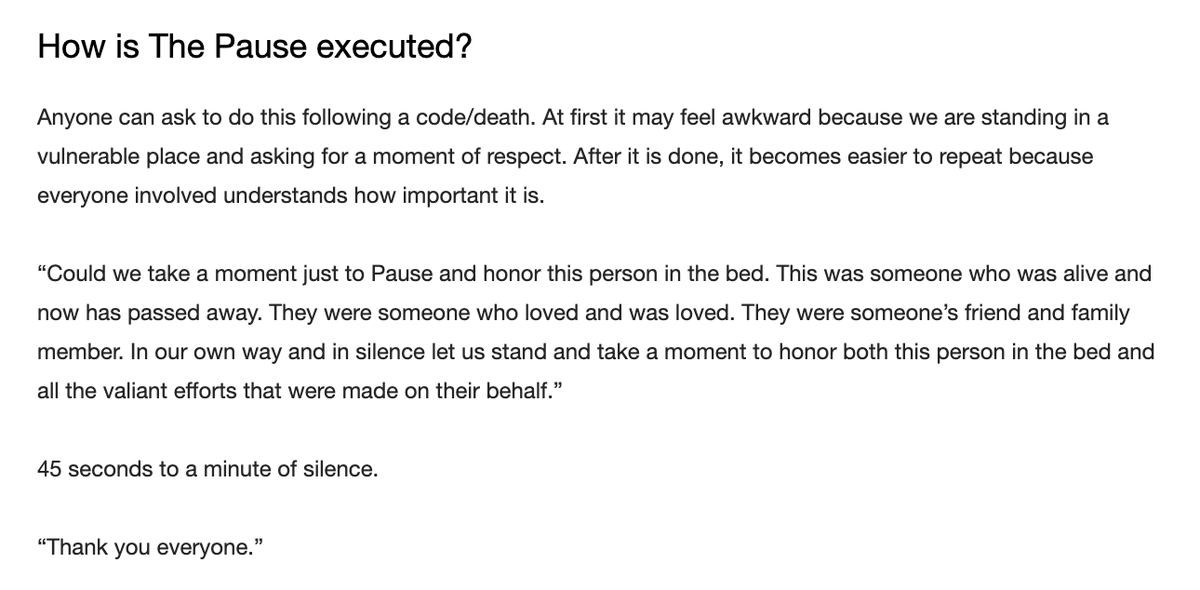
I am grateful for the Pause our ICU nurse in charge conducted today after the death of a patient. Apparently the first one done on this Unit. Meaningful for all staff present. Interested to hear who else is doing this in their EDs & ICUs.
53
281
2K
A beautiful CMAC video. It shows the visual representation of the 'clicks' you feel when the coudé tip of the bougie bounces over the tracheal rings, like a kid dragging a stick along a picket fence.
28
412
2K
Extubation Readiness: A to L Checklist. We're obsessed with safe intubation, but what about taking the tube out?. How do we assess extubation readiness?. Here's my simple, alphabet-based A to L checklist:. 1/17

21
457
2K
Recently on ICU. Me (to team): this lady no longer requires any critical care. Get her back to the surgical ward asap. Senior nurse: Cliff I don't know what it is but I'm worried about this patient and don't think she should go to the ward. Me: this patient is staying on ICU.
34
135
1K
The iGel is a great supraglottic airway device. But like other supraglottic airway devices (SAD) it's not foolproof. Here's how to maximise your success with the iGel - a thread 🧵
50
544
1K
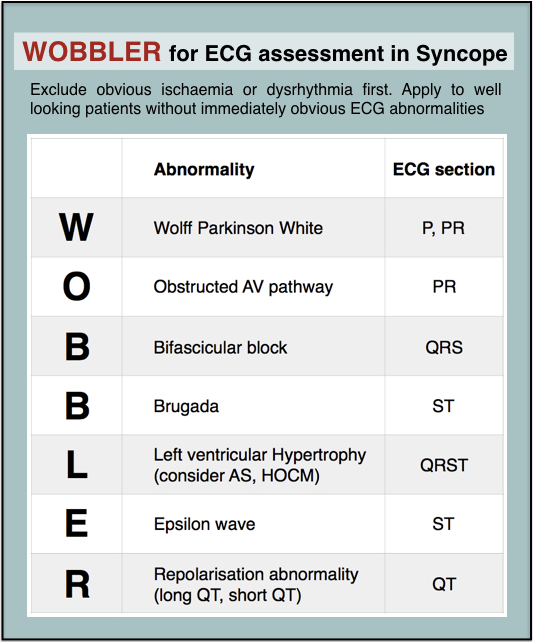
How I review ECGs of syncope patients to avoid missing the rare stuff. The 'WOBBLER' approach.
6
345
1K
What are your ‘famous last words’ at work?. I’ll start: .“I’ll just quickly see this elderly patient before I go home”.
188
35
1K
Night ED registrar: Sorry to wake you Cliff. I’m in resus with an 11 year old boy who. Me: Before you go on, are you phoning for advice or would you like me to come in?. Reg: Can you come in?. Me:
32
40
1K
Here's a reflection on how the management style of the emergency physician in charge (EPIC) can mean the difference between life and death. (Long 🧵).
33
334
1K
Hospital design committee sometime in the past. “Let’s get boxes of clinical gloves that open on top, and mount them with that surface vertically. This way, when a clinician pulls out a glove, an additional three will fall on the floor”. “Great idea - motion passed! What’s next?”.
33
77
968
Over the last couple of decades my colleagues and I have analysed HUNDREDS of resuscitation cases and here are the THREE things you need to master to save more lives.
10
284
943
Some maths. Intelligent & experienced doctor. Bullying dickhead.=.Bullying dickhead. Colleagues, your professional status & lifelong contribution to medicine does not entitle you to abuse others, no matter how much that short term buzz compensates for your personal inadequacies.
11
201
891
Want to improve your Basic Bag-Valve-Mask Ventilation skills? Here's a VERY short course I made that's free and will only take 5-10 minutes.
11
305
854
Why is it that whenever some dude over 60 goes off to get his prescription for dabigatran or rivaroxaban it always seems come with a free ladder?.
18
51
760
Because of modern slang it's hard to know when someone describes an ECG as 'fast AF' whether they're commenting on the rhythm or just a very fast rate.
27
66
762
When the emergency department becomes the final common dumping ground for the consequences of health and social system failures and lack of alternative services…. … emergency medicine neither contains much emergency nor much medicine.
14
154
738
.@Apple one thing you could do to help us when we're busy fighting the pandemic is stop iPhones autocorrecting 'Fuck' to 'Duck'. I really don't have the time.
20
104
725
On New Year’s Day at an Emergency Department in Sydney one of my colleagues received a call from the bed manager to say there are no beds so can they please try to send home any patients that don’t need to be admitted. Posting here to spread this ingenious novel practice idea.
38
70
726
Please read this thread to better understand how to interpret a high lactate. This patient had a CT to look for mesenteric ischemia because of the high lactate. However they clearly are ALKALEMIC due to HYPERVENTILATION. This is not a lactic acidosis- it’s a LACTIC ALKALOSIS.
Age 50 abdominal pain & vomiting. Looks well. No peritonism. How worried are you about ischaemic bowel?

27
152
720
Emergency physician’s pulse:. Seizing child - 56.Surgical airway for GSW to face - 64.Rapid tranquilization of psychotic patient on ice - 68. “Pain everywhere for 3 months” - 104. “Our naturopath said not to immunize our child” - 120. “You know that patient you sent home?” - 180.
11
156
676
Local radiologist has opened a takeaway. “Hi! I ordered a curry”. “You REQUESTED a curry”.
19
46
665
Doctors come & go. Resus NURSES are the best potential source of continuity & consistency of how resuscitation is provided in the ED . Invest in them & they become dependable guarantors of quality, safety & excellence. But only if supported & empowered by the medical leadership

10
136
632
We receive almost daily reminders of the fragility and temporality of human life, and yet continue to delude ourselves that we’ll ‘take some time off next year’ or ‘go travelling one day’ or ‘work long hours now to save for retirement’. Wake up. Live your life. TODAY.
20
271
608
Elevated lactate keeps getting misdiagnosed as 'sepsis' or 'ischaemic gut'. Even by smart people in fancy places. So I'm reposting this video so the resus nurses & residents & medical students can help their senior colleagues think beyond these two causes.
7
204
611
Hey anyone around in Britain in the late 70s? Did they ACTUALLY make primary school kids do gym stuff in their vests and underpants or is this a false memory?.
571
15
576
Remember that giving peripheral norepinephrine/ noradrenaline, proven in multiple studies to be safe, can cause some intensivists to become necrotic and fall off.
21
71
551
1/3 Here’s today’s dose of awesome. Saturday evening visit to the ED by the interventional cardiologist with printouts of before & after angios from the two patients we sent him today so we can relate the pathology to the ECGs and find out how our patients are doing now
16
48
556
Me: 2 packs of diclofenac please.Assistant: you can only have 1.Pharmacist: we’re not allowed to sell 2.Me: it’s not a drug of abuse and an overdose of 2 packs probably wouldn’t harm me.Pharmacist: okay have 2.Assistant(scans box): good news these are 2 for the price of 1 today.
24
28
545
Three #cardiology cases with diagnostic ECGs in our resus room today and some learning points for emergency clinicians. #ecg #ekg.
15
150
557
Muppet GIFs to correspond with medical specialties please.
267
184
538
For a sustainable career in emergency medicine, my #1 tip to emergency medicine trainees is don’t do it full time.
26
44
524
Some of my more controversial beliefs about anti-inflammatory drugs are probably best left nsaid.
10
30
519
Crashing or Arrested Pulmonary Embolism. Quick Reference Guide I made for MY OWN practice in non-ECMO centres without access to inhaled nitric oxide or other specific pulmonary vasodilators. Evidence base = thin.Official endorsement = none.Experience = limited. Not for junior
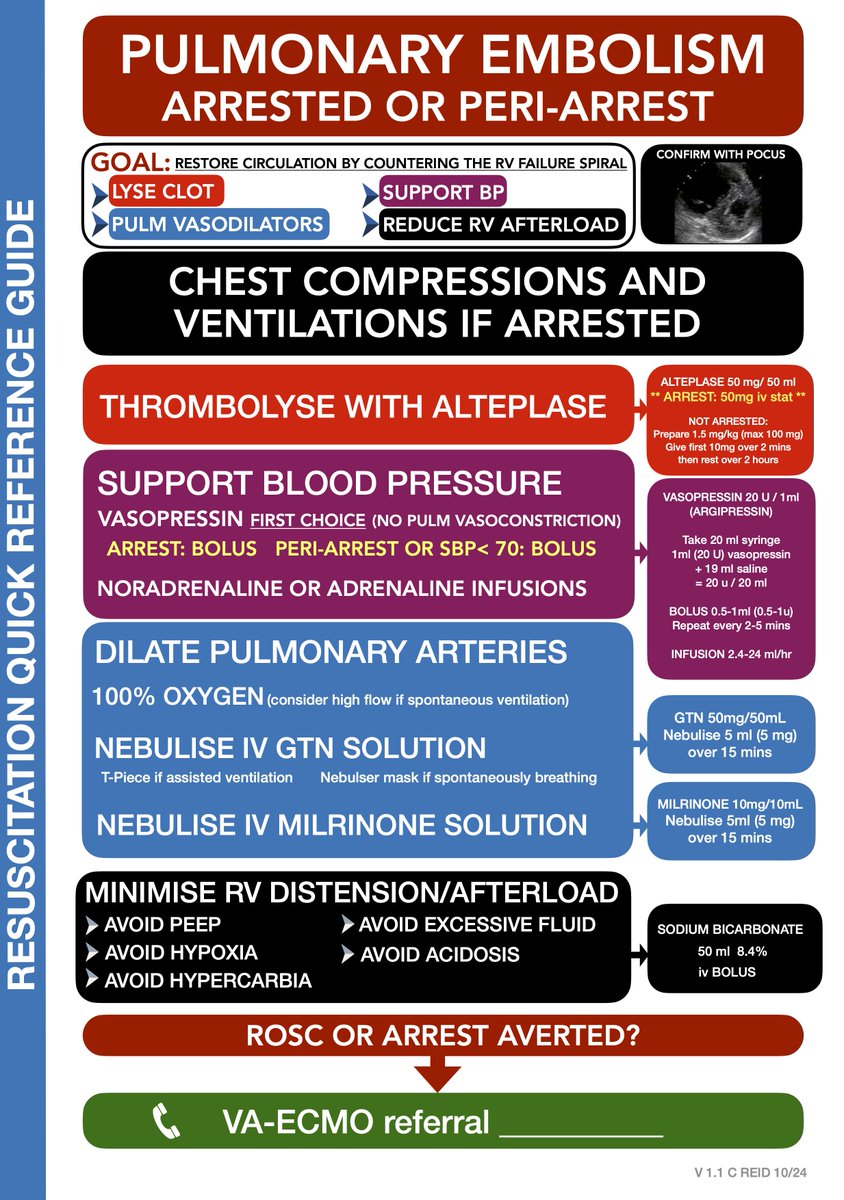
12
146
554

I don’t think supraglottic airway insertion is adequately taught to non-anaesthetists (including paramedics and EM people). The assumption seems to be that devices like the iGel are foolproof but that’s not the case. I feel a deep dive thread coming on soon.
45
27
496
Four ways to get better at sepsis management in the ED and save more lives. - a thread 🧵.
6
148
495
Everyone training in Surgery, Emergency Medicine and Critical Care please repeat after me:. A normal lactate does NOT rule out ischemic gut. There. Now write it out 100 times.
22
51
458
Brave RN goes out to 'pacify' the waiting room with an update on waiting times
6
34
451
Finally to your relief the night ED registrar arrives and takes a moment to review the waiting list and the state of the department you’re handing over
9
17
441
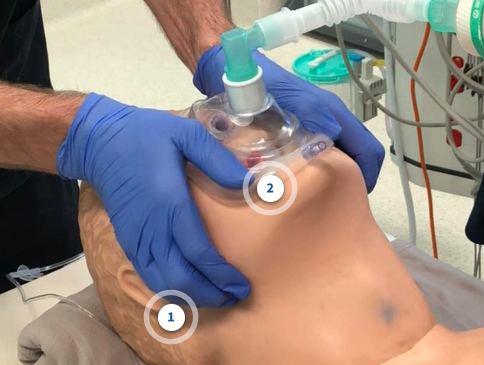
Quick Free Airway Education!. Taking time to correctly position a patient is, in my view, the NUMBER ONE way to improve your chances of successful airway management. I've made a short (5 min) free lesson. Please have a look and give your feedback after.
27
143
443
Remember: anyone who is task-focused on a procedure loses situational awareness. Try to be hands-off as team leader otherwise anything could be going on around you.

12
238
435
Remember the old days when it got busy in the ED and you rolled up your sleeves & said ‘Righto chaps let’s smash this queue!’?. Now with thirty 90+ year olds sent from nursing homes with frailty, multimorbidity & polypharmacy & no advanced care plan, the queue smashes YOU.
17
28
438
Major GI bleed.Massive PE.Cardiac tamponade. all referred to ICU with ‘septic shock’ by normally reasonable ED docs thanks to this EMR alert. a negative consequence of well-meaning systems design. Nudging clinicians towards a diagnosis of sepsis creates false positives
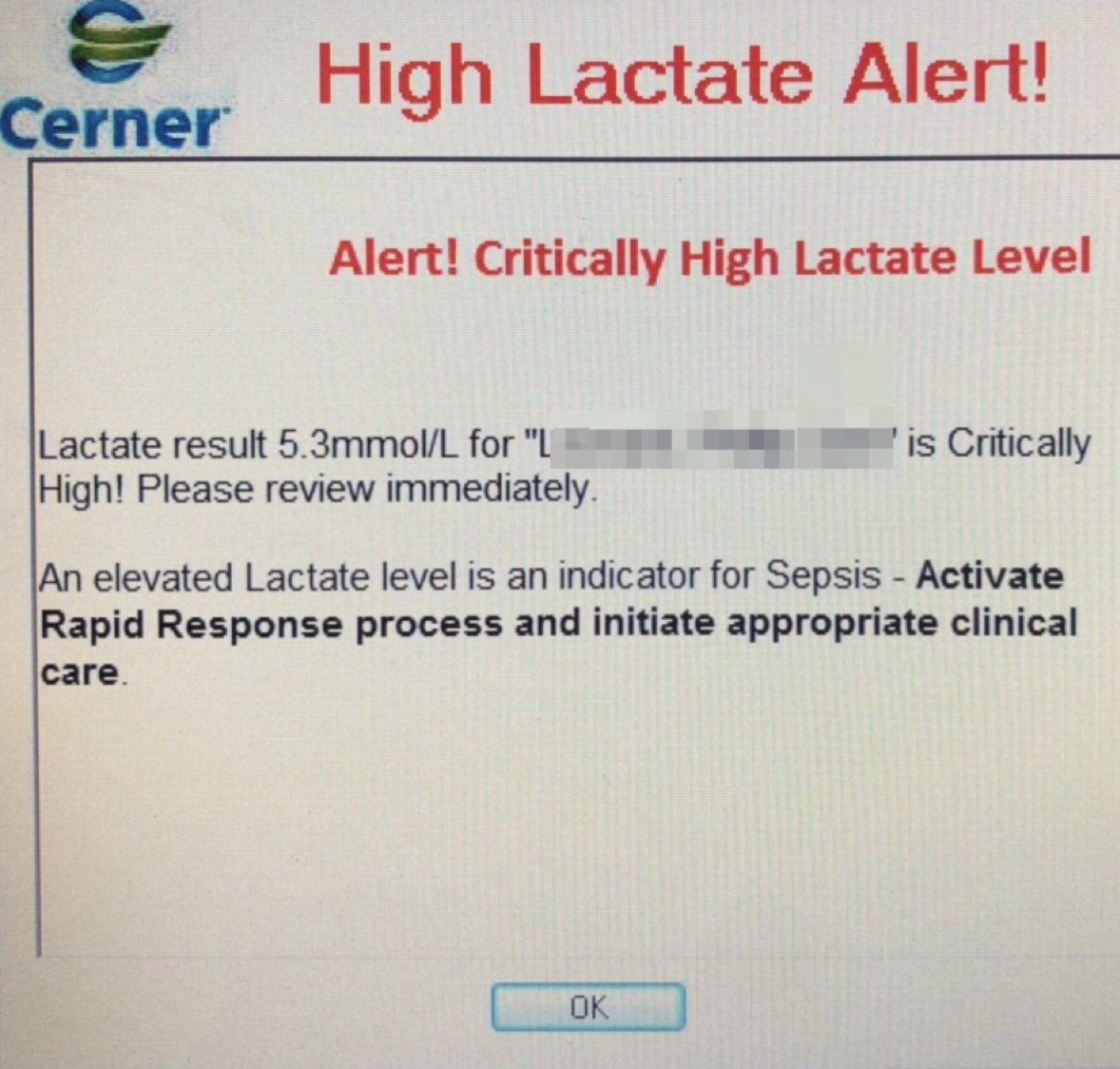
37
78
430
Called in from home at 0530 by nurse in charge of ED for super sick young patient. On my arrival (less than 20mins later) team had everything necessary already sorted to stabilise the patient. It could be argued I made very little difference.Couldn’t be prouder.
9
6
424
Never take your EYES off the PRIZE!. During direct laryngoscopy.the assistant should be trained to hand the bougie so the operator doesn't have to look away from the airway. To do so risks losing the view
7
48
427
If you're not a paramedic but you think you know what they do, PLEASE read this. I think everyone in healthcare should read it, but ESPECIALLY emergency medicine and primary care clinicians. 1/.
17
164
399
I'm sorry, but NO. I've looked this up. There aren’t many case reports but those that exist show that intravenous gasoline causes tissue necrosis, severe lung injury and multi organ failure, often leading to death.

Yep. To quote @PMHTrauma_ALE for the 722nd time. "The only pre-hospital fluid a patient needs is diesel.". In other words, get the patient to the hospital!.
25
40
400
Our hospital opened at the end of October 2018. Since day 1 of opening we have kept a detailed registry of all intubations in the emergency department. We completed our sixth year of data collection this week. 1/14
27
75
412
This has to be the core mission of the Emergency Physician in Charge, and we should seek neither permission nor forgiveness to discharge this responsibility to the best of our ability. End of 🧵.
15
23
398
The surgeon takes a patient with appendicitis to the operating room based on history and clinical exam findings
8
15
382
Just in case anyone still thinks ketamine elevates ICP. “Ketamine was associated with a reduction in ICP….If these findings are reproduced. , ketamine may warrant consideration as a treatment for intracranial hypertension in children with severe TBI”.
9
131
405
🧵 Managing Challenging Behaviours in Resuscitation Teams: A Thread for Team Leaders (1/13). Every resuscitation team leader can face difficult team dynamics. Here are 6 key challenging behaviours you'll encounter and how to manage them effectively in real-time 🚨

9
162
416
Age 50 abdominal pain & vomiting. Looks well. No peritonism. How worried are you about ischaemic bowel?
67
62
395
1/.My favourite three Powerful Magic Words to disarm any clinician from another specialty who for some reason thinks it's okay to yell at your staff:. "Who are you?".
10
38
366
I propose an important new hypothesis on ED human factors paraphysiology, as a non-peer reviewed pre-print. Feel free to cite this Tweet in your academic commentary. This is how science works now post-COVID.

14
80
382
Stopping someone from bleeding to death requires many keys steps. Our team uses this cognitive aid. Page 1 covers general measures to guide vascular access, haemostatic resuscitation, reversal of anticoagulation, and optimising of clotting. 1/10

5
158
390
Patients with acute life threatening pathology often feel the need to open their bowels urgently. Paramedics recognise this as a potentially very important symptom. I call this the ‘Death Dump’ or ‘Pre-terminal Turd’. Probably one of the reasons so many arrests happen in toilets.
22
43
373
The most dreaded words in emergency medicine:. “You know that patient you saw…”.
11
38
378
Essential microskill for airway assistants!. When intubating over a bougie, the bougie is placed into the trachea and the assistant places the tube over the bougie. Because bougies are straight and tracheal tubes have a curve, there is a tendency for the bougie to hit against the
12
92
395

Agitated peri-arrest pt required urgent central access for renal replacement. I asked for ketamine/midazolam but resident held patient’s hand, reassured her & no sedation needed. In the debrief I described him as ‘human ketamine’. Does he realise there is no greater compliment?.
11
33
371
1/ Emergency front-of-neck access is not a ‘failed airway’. It’s an alternative airway, and therefore a ‘successful airway’. Terminology matters, as it frames our mental models, which influence our behaviour.
16
49
367
Last night we had a case that demonstrates an extremely important cause of shock that many ED clinicians know little or nothing about. 1/.
9
103
361
The European Society of Emergency Medicine has published new recommendations on Emergency #Airway Management 🧵.
4
96
370
Doris' dislocated hip prosthesis went back in easily but we might have overcooked the sedation for a 55kg 90 year old
3
8
351
Always take into account the cultural and linguistic background of your staff when communicating medical orders. For example we have a nurse from ancient Rome who gave my patient four paracetamol tablets because I prescribed it IV.
10
25
344
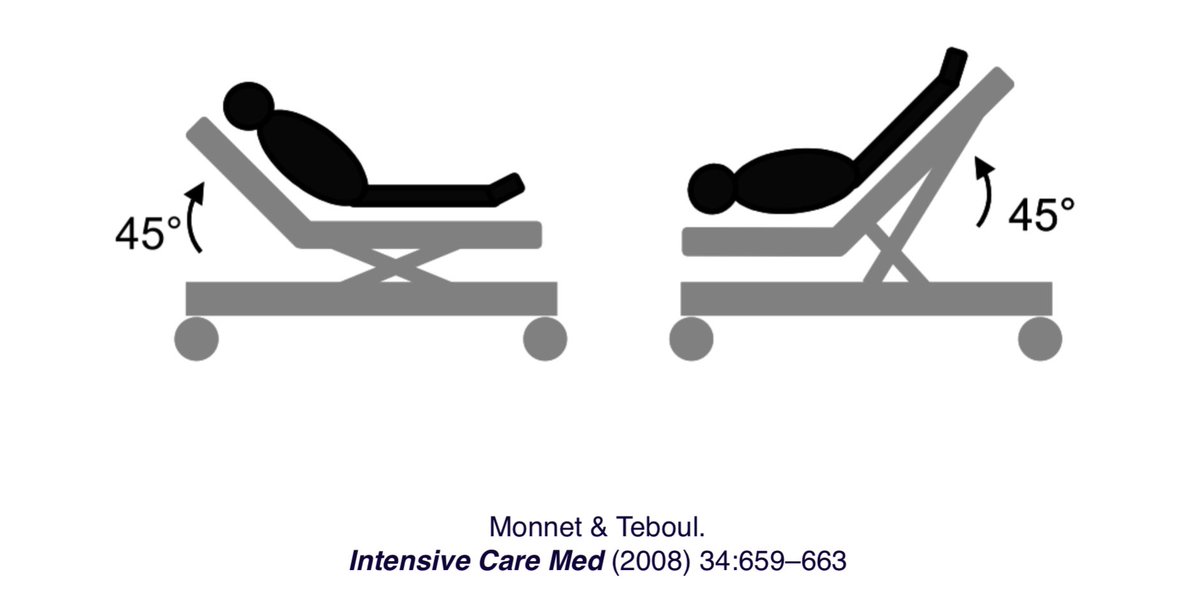
By all means try a Passive Leg Raise as a ‘fluid challenge’ if you want, but have the head and body flat, not tilted down, and be clear what your end point is.
4
50
359
If a trainee has first look at direct laryngoscopy, it's our responsibility to coach them through to first pass success, rather than take over. This is how they learn to troubleshoot, rather than believe some airways are too difficult for them. CMAC is perfect for this.
17
45
360

First draft of a PROPOSED pathway for identify 'happy hypoxic' #COVID19 patients at triage, and giving them a chance NOT to get intubated. Work in progress. Very interested to hear from anyone with something similar/better in place. No experience of these patients yet

23
153
355
The hospital 'wellness program' recommends capitalising on opportunities to breath fresh air outside so you pop out to the ambulance bay and have a moment to yourself
5
11
334
I don’t know who needs to hear this but there are other potential sources of sepsis than the chest and urinary tract.
30
26
335
New intern orders the nurse in charge to 'fetch' something for him
6
11
335
Lots to remember to do as a patient tries to bleed to death. Here's the front of our haemorrhage control cognitive aid for use in the resus room.

12
129
333
When intubating critically ill patients, please do the OPPOSITE to the things on this list
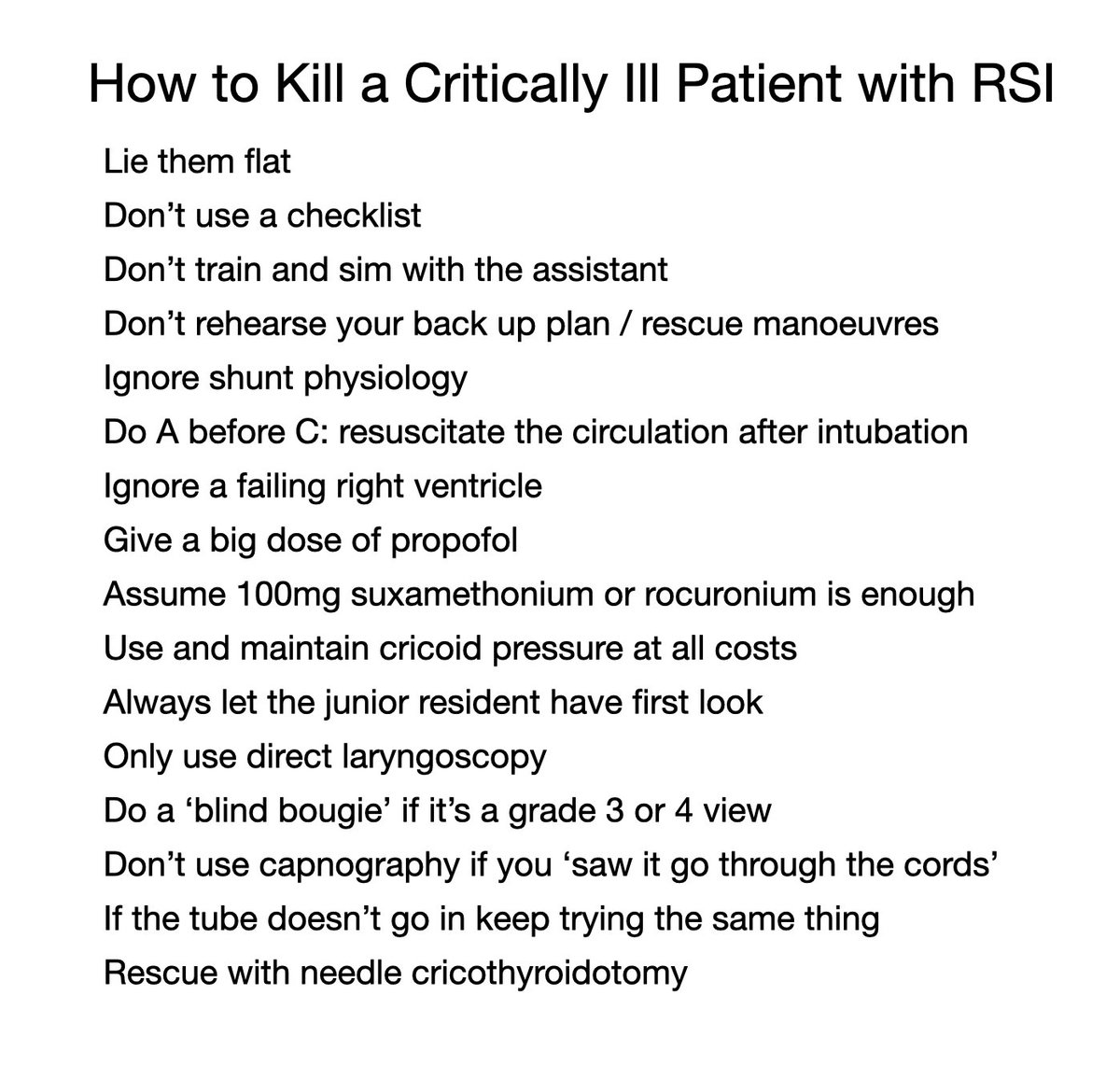
10
128
348
Doctor Team Leader: “Right everyone let’s have quiet please this patient is sick and we need to focus. I want you to…”. Team: “He’s such a strong leader”. or. Team: “She’s such a bossy bitch”.
9
46
331
If your job includes reading ECGs in patients with chest pain, this will be one of the most useful hours you'll ever spend in your career. Trust me on this. via @smithECGBlog.

Lecture by Smith: Selected Cases of Occlusion MI (OMI), or not, on the ECG.
1
77
339
Very short🧵on AF in hospital 1/5. Atrial fibrillation in hospital often starts from interplay between underlying risk factors (substrate) & acute triggers

1
104
342
One of the signs of maturing as an emergency physician is accepting there are situations where more care by me is less useful to the patient than getting them to the right specialist team sooner rather than later. The best paramedics also go through this.
11
28
316
A recent discussion was around ‘who does the airway belong to in a resus situation?’. I have very strong views on this. It belongs to the patient. Your system should be set up so that the patient’s own airway is managed as effectively as possible. And that takes a team.
9
104
325
Early 40s male with chest pain and collapse, looks horrible, SBP 80, lactate 7. Previous large PE with pulmonary hypertension on echo 2 months ago, discharged on apixaban.POCUS on arrival shows:



19
95
336
Even if you remain unconvinced that video laryngoscopy improves your likelihood of first pass intubation success, why would you NOT want to share this view with the rest of your team? Airway is a team sport and the airway assistant and team leader seeing this keeps things chilled

18
35
322
WOBBLER - identify critical ECG abnormalities in the otherwise well looking syncope patient, going in PQRST sequence.

3
268
330
Seven hours into the shift you know there’s going to be no time for a meal break so you steal some jelly from the paeds ED fridge. This provides an opportunity to reflect on the shift so far
1
9
317
Before you anaesthetise your next head injured patient, just a quick reminder that ketamine isn’t harmful, but hypotension is.
10
38
313
Emergency care is broken. Patients suffer long waits, inadequate warmth, hydration, analgesia, privacy and dignity. The Emergency Department can't provide all the things patients and other health care workers expect of it. At some point we need to be honest about that.
2
64
309
Surviving as a team leader in emergency medicine. Here are 10 learning objectives & strategies I recommend:. 1. Develop a resuscitation mindset, taking responsibility for the critically ill patients under your care. - ownership is key
1
108
315
And on today’s edition of ‘Resuscitation - DID YOU KNOW?’. Arterial and central venous catheters are great but they’re not actually treatments. If someone’s critically ill and deteriorating there are higher priority issues that shouldn’t wait for the lines. Just sayin’.
33
35
295