

Sameed M
@_MSAMEED
Followers
2K
Following
2K
Statuses
6K
Pulmonary & Critical Care @ClevelandClinic. #FOAMed. 🏴🇵🇰🇺🇸Tweets reflect my personal opinion. #pulmCC.#PH #ILD #SEVAmaster
Cleveland, OH
Joined April 2013
@OfVentilation I think recognising early cycle is relatively easy how to adjust ventilator/sedation to avoid it is hard
0
0
3
Review of the HAPPEN Randomized Clinical Trial, which evaluates the effect of high-intensity vs. low-intensity noninvasive positive pressure ventilation (NPPV) on the need for endotracheal intubation in acute exacerbations of COPD with hypercapnia. 🔹 Methodology Review ✅ Strengths: • Randomized, multicenter design across 30 hospitals enhances external validity. • Defined inclusion criteria (PaCO₂ > 45 mmHg after 6 hours of low-intensity NPPV) ensure that only patients with persistent hypercapnia were included. • Crossover allowance for the low-intensity group reflects real-world clinical scenarios. • Clear intervention protocols for high- and low-intensity NPPV with detailed titration strategies. • Blinded outcome assessors enhance objectivity in determining the need for intubation. ⚠ Limitations & Concerns: • Single-blind design: Patients and treating physicians were unblinded, potentially introducing bias in decision-making regarding intubation. • Early trial termination due to interim analysis findings and COVID-19 disruptions may have impacted long-term conclusions. • Potential confounding from prior NPPV use: Over 55% of patients had used NPPV before, which might have influenced treatment response. • Limited generalizability: The study population was older (mean age 73 years) and primarily from Chinese hospitals, which may not fully translate to other healthcare settings. 🔹 Statistical Analysis Review ✅ Strengths: • Intention-to-treat analysis ensures robustness by including all randomized patients. • Predefined superiority margin (9% absolute difference in intubation) maintains statistical rigor. • Multiple sensitivity analyses (e.g., per-protocol analysis, adjustments for baseline characteristics) reinforce findings. • Kaplan-Meier and Cox regression models for time-to-event analyses strengthen interpretation. ⚠ Concerns & Weaknesses: • Primary outcome (intubation need) had a significant difference, but actual intubation rates did not (4.8% vs. 13.7% met criteria, but only 3.4% vs. 3.9% were intubated). This suggests that while high-intensity NPPV prevented patients from meeting criteria, it did not necessarily reduce actual intubation rates—raising questions about clinical impact. • 1-sided p-value for primary outcome (P = .004) rather than the conventional 2-sided approach. This increases risk of overestimating statistical significance. • Adjustment for multiple comparisons: The study analyzed 15 secondary outcomes, but only 1 was significantly different, suggesting possible chance findings. • Post hoc subgroup analyses were exploratory and not sufficiently powered. 🔹 Conclusion & Clinical Impact ✅ Key Takeaways: • High-intensity NPPV reduced the proportion of patients meeting intubation criteria. • No significant difference in actual intubation rates or mortality. • Increased abdominal distension in high-intensity NPPV, suggesting potential tolerance issues. • High-intensity NPPV achieved better PaCO₂ reduction, but long-term benefits remain uncertain. ⚠ Limitations in Conclusion: • The crossover design may have diluted differences, making it hard to conclude whether high-intensity NPPV is truly superior. • Did not address long-term COPD outcomes, such as exacerbation frequency or readmissions. • Results conflict with prior studies suggesting high-intensity NPPV improves survival in chronic hypercapnic COPD. 🔹 Final Verdict ✅ Well-designed study with strong methodology but some limitations due to unblinding and early termination. ⚠ Findings suggest high-intensity NPPV improves gas exchange but does not clearly prevent intubation or improve survival. 📌 Future studies should assess long-term outcomes, patient tolerance, and cost-effectiveness.
0
1
11
Asking for my learning, is there a good place where one can verify the copay and coverage of medications that we prescribe to our patients. I have found the EMR integrated prompts to be accurate only 50% of the time. #HealthcareInnovation
1
0
4
Probably the most comprehensive, and compete course to become a master in Mechanical Ventilation

SEVA program on mechanical ventilation registration now open ! Here are the dates for 2025. Join us in our path to getting better. @CCF_PCCM @ClevelandClinic @medpedshosp @msiuba @OfVentilation @_MSAMEED @RaedDweikMD @ArielG_RRT @chatterJ5 @Thind888
0
0
5

@GloriaSong88 @ummidtownim @UMMC @Abdellatif_07_ Amazing residency program filled with amazing residents. Missing the holiday vibes #Midtown
0
0
7
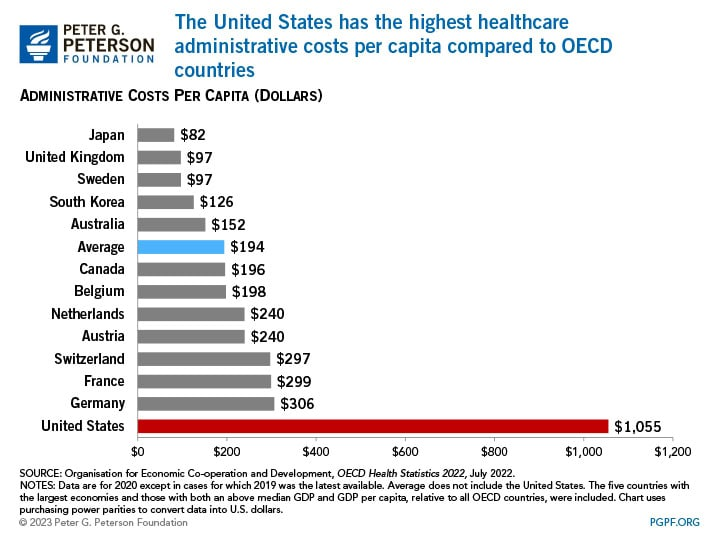
All this admin cost to actively find ways to delay or deny care to patients.

The United States has the highest healthcare admin costs (per capita) compared to OECD countries.
0
0
5
Proud Mentor moment, all my mentees matched at their desired PCCM programs
0
0
46
@ArielG_RRT @emireles_c @CCF_PCCM @DocMusician @IM_Crit_ @critconcepts @OfVentilation @ATC_Ventilator @SaudiRTs @Vent_Busters @Srivatsa34 @HibaVentila @DrMiguelIbarra1 @RespiratorySCCM Makes, sense I support all efforts to work the diaphragm. Especially when the aim Is comfort. The curse of not being at the bedside when doing vent waveform analysis 🧐 Great waveform
0
0
1
We concluded our fellowship interviews last week, an excellent group this year. One pattern I noticed is the introduce yourself question - the answers were excruciating long, taking time away from the actual conversation. Practice a short but concise introduction. Next would be the #Match2025 residency interviews. @Inside_TheMatch
5
8
164
Excellent vent education with high quality pearls from @emireles_c available on @YouTube
5 more episodes SEVA VentRounds Leaks, failed trigger, expiratory effort and other cool stuff... @CCF_PCCM @YalePCCSM @JHUPCCMFellows @UCRCriticalCare @UCLAPCCM @UChicagoPCCM @msiuba @_MSAMEED @MegriMohammed @Thind888 @vic_puente @DrMiguelIbarra1
0
0
2
@medpedshosp @AndreMansoor @CCF_IMCHIEFS @AndreiBrateanu @Mud_Fud If I had this book in med school it would have accelerated my learning my years. Still hoping to get me copy signed from @AndreMansoor
1
0
3
Dear Mustafa, Thank you for highlighting a sore truth, we as IMGs got here today because of the altruism of many other IMGs and US physicians. To use the vulnerability of an IMG and charge them is a horrible new trend. Same goes for charging humungous amounts for very poor perception in the name of USCE, and post pandemic there is a new influencer space that targets IMG applicants in particular. As someone who has been an applicant and now on the other side as core faculty in a program, I can attest to you a resident or even a fellow don’t have the exposure to know about the recruitment process. #Mentorship @Inside_TheMatch

People who extort IMGs by making them pay to review their PS are the worst. Also just because you matched doesn’t make you an expert in the match and how to write personal statements.
1
6
119
