

The Journal of Arthroplasty
@JArthroplasty
Followers
14K
Following
5K
Statuses
2K
The Journal of Arthroplasty brings together the clinical and scientific foundations for joint replacement of the hip and knee.
New York, NY
Joined June 2017
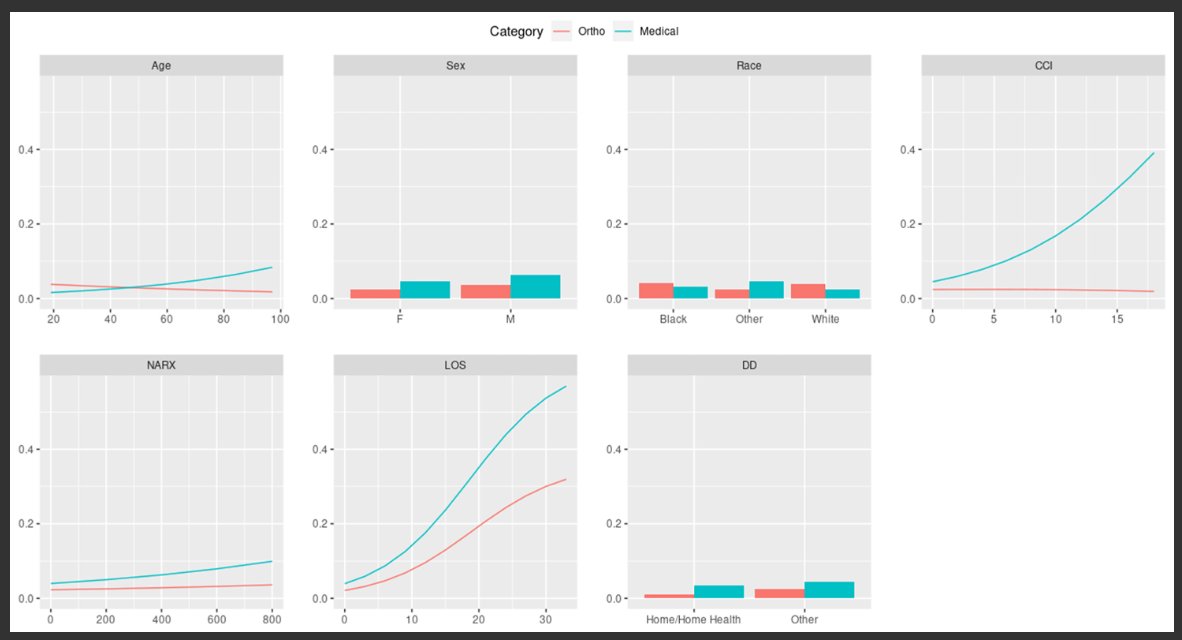
Through successfully constructing and validating multiple 90d readmission predictive models, this study highlights the distinct risk profiles for medical and ortho-related readmissions.
0
0
0
More women ortho surgeons are matching in adult reconstruction, but the % of women adult reconstruction fellows has been stable, highest in 2021. Women’s membership in AAHKS is encouraging, especially at the resident and international levels.

0
0
8
This study showed a novel screening gait test at 6wks shows promising results for predicting patients who will likely have poor recovery based on at least one gait parameter recovery curve at 12wks with high sensitivity and specificity.

1
2
5
Although ASCs have strict patient criteria for SDD TKA, complex patients at a tertiary university hospital can be sent home the same day with equivalent outcomes.

1
0
3
The IA-triamcinolone extended release appears to outperform other treatments in terms of pain relief and functional improvement for up to 4mo following treatment for knee DJD.

0
2
13
Tantalum concentrations in rTHA were significantly higher in patients who had the implants compared to controls; however, the systemic and local effects of an increased tantalum exposure are not yet fully understood and have to be further investigated.

0
7
34
Smart TKA implants with sensor technology embedded within the implant can record data that tracks recovery. This study of gait metrics and step count found the screening gait test at 6wks can predict patients who will likely have poor recovery at 12wks.

1
2
13
This study showed among patients who have depression, antidepressant therapy before TKA or THA is associated with improved outcomes. Additional studies are needed to establish the impact of interventions to address untreated depression before surgery.

1
4
19
rTJA with unexpected positive intraoperative cultures were not significantly associated with a higher re-revision risk at 5yr. Those revisions performed within the first 24mo after primary arthroplasty had a higher rate of any-cause failure.

0
0
4
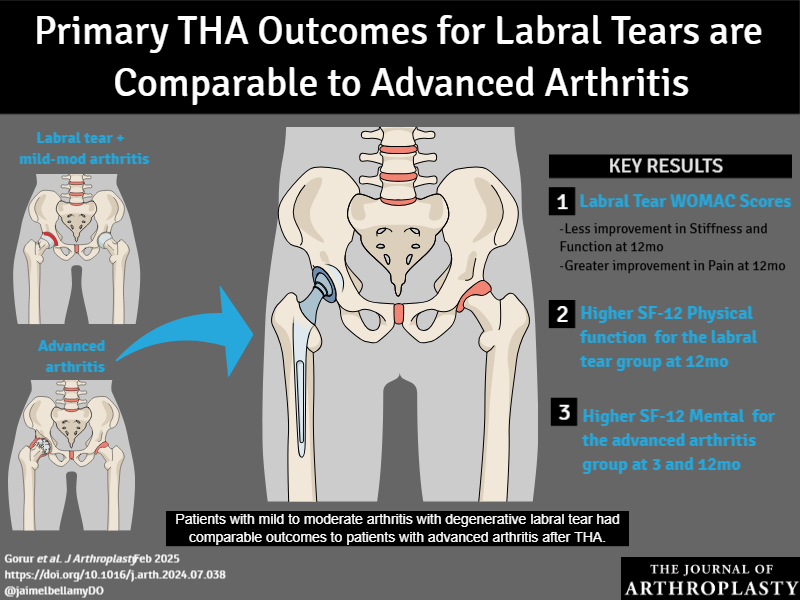
Patients who have symptomatic degenerative labral tears with mild to moderate arthritic changes have comparable outcomes to patients who have advanced arthritis following THA.
2
21
99
Medically optimized patients categorized as ASA 3 can safely undergo SDD TJA without increased risk of 24hr or 90d complications. Patient preference for outpatient DC, reliable social support, and independent functional status are imperative for success.

0
2
2
Press Ganey Surveys were higher in patients who received flowers from their surgeons compared to patients who did not, and the scores persisted if the patient received flowers. The gift of flowers generates patient loyalty to their surgeon.

0
0
2
RCT bilateral simultaneous TKA: Anatomical and mechanical alignments had similar clinical outcomes in patients undergoing bilateral total knee arthroplasty at a mean of 4.9 years follow-up.

1
19
88
Medicaid insurance is a risk factor for increased total complications and LOS following TKA. Appropriate preop/periop management of these patients is essential in order to mitigate the risk and burden on the health care system in this population. *Link in bio

0
0
4
Patients who have EDS possess significantly higher odds of complications after THA compared to matched controls, including dislocation, aseptic loosening, and aseptic revision. Careful surgical planning is required.

0
1
4
This model showed preheating time, volume of flushing fluids, the intraop infusion volume, the anesthesia and surgical time, and the core temperature after intubation could accurately predict intraoperative hypothermia in TJA patients.

0
0
1
Starting up a lateral UKA practice is safe and efficient for surgeons who have prior medial UKA experience, provided strict adherence to indications. Surgical duration indicated a learning curve over approximately 33 cases.

0
2
5
Obese patients who underwent bariatric surgery prior to THA experienced reduced medical complications at all time points and reduced rates of revision at 72 months relative to a matched cohort who did not undergo bariatric surgery.

0
4
17
Clinically relevant HOOS-PS and KOOS-PS improvements are likely overestimated, as nonrespondents had higher adverse event rates which were associated with lower likelihood to achieve clinically relevant HOOS-PS and KOOS-PS improvements for TJA.

1
1
6
Women had an increased incidence of cemented femoral components (indicated for osteoporotic bone) and postop fractures. Women’s PROMs demonstrated globally lower functional scores and higher pain preop.

0
0
2