
Brad Gallent, MD, PhD
@DrGallent
Followers
44
Following
1
Statuses
36
Physician-scientist designing targeted therapies for prostate and other cancers to improve outcomes for our patients. Oncology Fellow @CSCancerCenter.
Joined September 2024
RT @TheCancerLetter: Cancer research fuels life-saving work, writes @CedarsSinai's Ze'ev Ronai.
0
5
0
RT @montypal: A meeting for my #SoCal colleagues. No lengthy travel required. Join us in #NewportBeach to discuss the current status of cli…
0
13
0
@jgong15 @MPishvaian @AnthonyNguyenMD Good point, in STAMPEDE (Arm H) 18% received docetaxel, as SOC evolved to include docetaxel for mCSPC as trial was accruing. I'd have to dig to see what percent of low vs high volume patients received docetaxel.
0
0
0
@MPishvaian @AnthonyNguyenMD Yes, STAMPEDE (arm H) trial showed OS benefit with RT to the primary given concurrently with ADT (vs ADT alone). We tend to extrapolate and give SOC ADT + ARPI (abi/apa/etc) while treating the primary. More studies are ongoing to evaluate.
0
2
2
Apologies, typo on the trial. Should be TITAN (with an A).
0
0
1
@MPishvaian Agree. Logically it makes sense treating the primary would have (more) benefit if you have less disease elsewhere. Nice when you have data to back up that gut-feeling.
0
2
2
@MPishvaian Correct. The common fusion is TEMPRSS2-ERG, where ERG is the oncogene partner. There is some preclinical data supporting ERG inhibition, but none in the clinic that I know of.
0
2
3
Great point/question. mOS is a little deceiving to compare here since the PEACE-1 data is separated between low and high volume. When PEACE-1 low and high populations are pooled their control arms (ADT + doce) have a similar mOS: 4.4 years (PEACE-1) and 4.1 years (ARESENS). PEACE-1 pooled mOS:

0
4
5
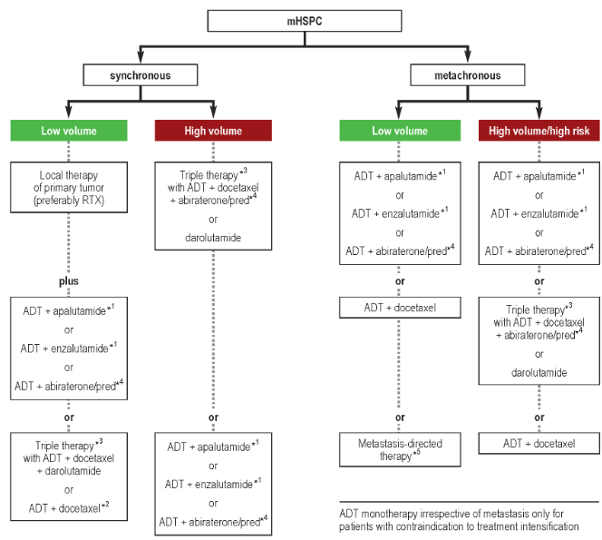
19/20 #TumorBoardTuesday Summary For low-volume mCSPC (mHSPC) Benefit for local therapy to primary tumor Benefit of metastasis-directed therapy (MDT)
0
4
11
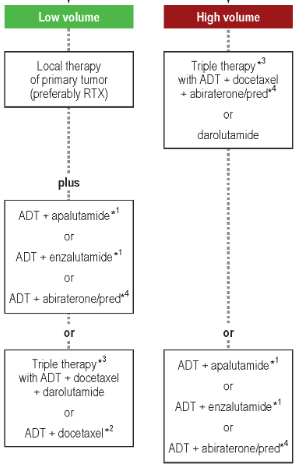
18/20 #TumorBoardTuesday Summary 1L mCSPC therapies stratified by volume High volume: Triplet therapies or ADT + ARPI (based on pt factors) Low volume: ADT + ARPI (based on pt factors)
0
3
9
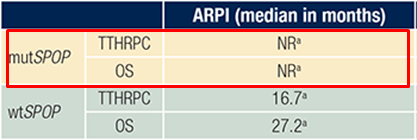
17/20 #TumorBoardTuesday Lack of an established biomarker to guide 1L therapies in mCSPC 🔬Studies ongoing, e.g. SPOP mutations 🧬may be predictive for ARPI + ADT
0
4
8
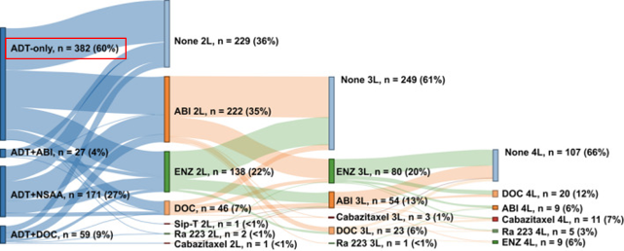
16/20 #TumorBoardTuesday Unmet needs in mCSPC ADT intensification underutilized in real-world studies Pts: mCSPC (2013-2018)
0
4
6
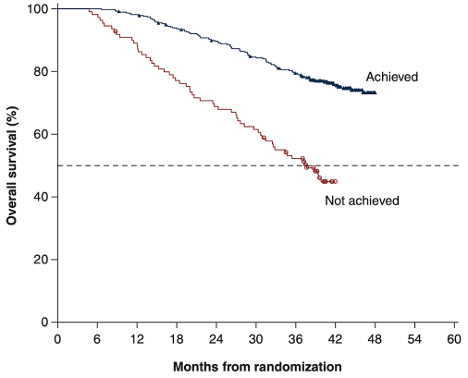
15/20 #TumorBoardTuesday 💡Mini tweetorial 7 Sig of rapid, deep, and durable PSA declines with apa + ADT Post-hoc analysis of 📚TITAN, median 44.0 mo Pts: mCSPC getting ADT + apa Achieved: >90% PSA decline or PSA <0.2 ng/ml at 3 months Median OS: 37.7 months “Not achieved” vs Not Reached “Achieved” (HR=0.35)
1
5
15
14/20 #TumorBoardTuesday 📋Back to our case 65M with de novo low-volume mCSPC Within 3 months, PSA <0.02 Interval NM bone scan/CT scan at 6 months shows stable sclerotic bone mets with resolution of activity in corresponding lesions🩻
0
3
5
12/20 #TumorBoardTuesday 💡Mini tweetorial 6.5 🔬Ongoing trials of MDT in de novo oligomets mCSPC (NCT03298087, NCT03784755, NCT03763253, NCT05223803) 📚 NCCN recs ⚡SBRT to oligometas from PCa when (1) goal is ablation (2) limited progression or (3) symptomatic lesion
0
3
6
11/20 #TumorBoardTuesday 💡Mini tweetorial 6 Evidence supporting metastasis-directed therapy (MDT) for oligomets Pooling 📚STOMP + 📚ORIOLE Pts: PCa recurrence low-volume met (no high-risk mut) Obs vs MDT (no systemic Tx) Median PFS: 7.0 months Obs vs 13.4 months w/ MDT
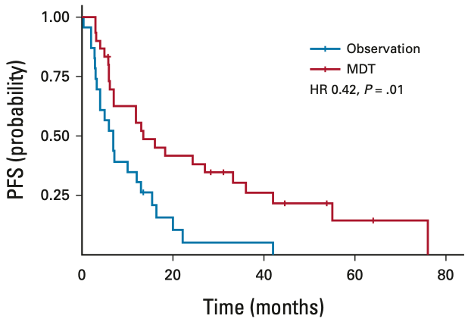
1
2
7