

Adam Bruggeman, MD
@DrBruggeman
Followers
2K
Following
516
Statuses
896
Spine surgeon, dual boarded in addiction medicine and orthopedics. passionate about health policy. AAOS Council on Advocacy Chair
San Antonio, Texas
Joined June 2014
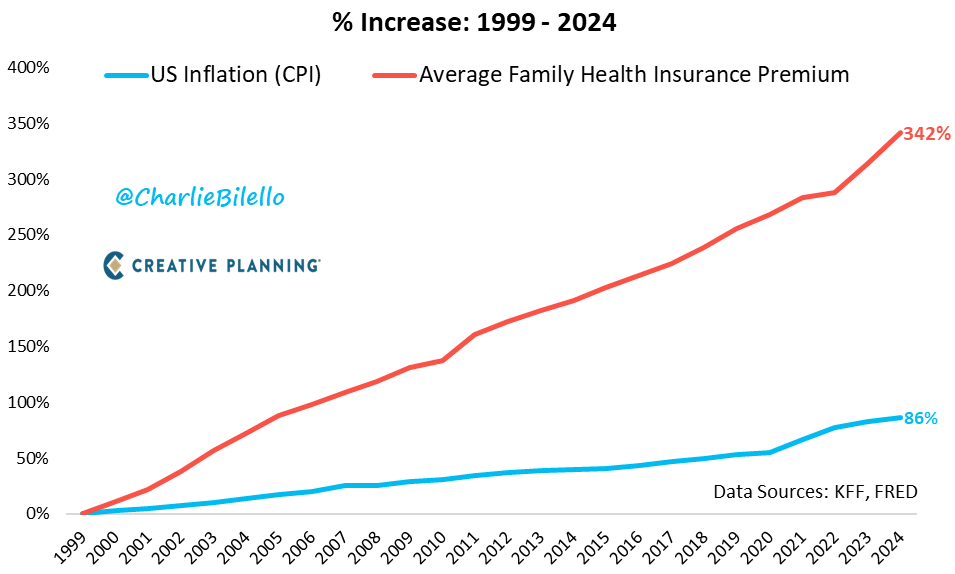
Physician conversion factors: 2000: $36.6173 2003: $36.7856 2006: $37.8975 2009: $36.0666 2012: $34.0376 2015: $35.7547 2018: $35.9996 2021: $34.8931 2024: $32.7442 UHC stock up 8,556% Insurance premiums up 342% Inflation up 86% Physician pay down 10% We should keep cutting physician pay so families have more money in their pockets through reduced costs and reduced premiums based on the last 25 years of experience.


Average US family health insurance premium... 2000: $6k 2003: $9k 2006: $11k 2009: $13k 2012: $16k 2015: $18k 2018: $20k 2021: $22k 2024: $26k That's a 342% increase since 1999 (6.1% per year). (Note: US CPI inflation has increased 2.5%/year)
55
275
818
@eric_novack I don’t know of any plans to increase doc pay over last 20 years. The only discussion is on adding inflationary updates going forward. As far as site neutral there are many concepts out there and it depends on how far they go as to the savings
1
0
1



Physician conversion factors: 2000: $36.6173 2003: $36.7856 2006: $37.8975 2009: $36.0666 2012: $34.0376 2015: $35.7547 2018: $35.9996 2021: $34.8931 2024: $32.7442 UHC stock up 8,556% Insurance premiums up 342% Inflation up 86% Physician pay down 10% We should keep cutting physician pay so families have more money in their pockets through reduced costs and reduced premiums based on the last 25 years of experience.
2
1
5
Wow and thank you…. While there are things in here that I think need some revising, this is incredibly well thought out and done. I would encourage physicians and health policy aficionados to read through this. This encompasses so much of what many have asked for!

Today, we launch “The Case for #HealthcareFreedom.” With @realDonaldTrump in the White House & @RobertKennedyJr at HHS, it’s time for bold, transformative change. Empower Patients & Doctors, not Insurance Companies & Bureaucrats. #HR317 #MAHA

0
0
5
@BeckersHR published an interview with @commonspirit CFO today. In it he complains that insurers are denying claims and making it more difficult to get paid. He also notes that it seems like there is significant consolidation in the markets, and the higher consolidated markets seem to have a worse problem. This is particularly bad within the Medicare Advantage system. He states that the denials are particularly egregious because hospitals will get them overturned the vast majority of the time (@TSAOG_Ortho showed that they are successful 99% of the time) This is precisely what physicians have been complaining about for years as the prior authorization problems continue to mount. I have provided graphics from the federal government outlining how much consolidation has occurred within health insurance companies. This consolidation is BAD for healthcare. It is forcing physician groups to consolidate by joining together or becoming employed by hospitals, insurers, or private equity. Congress must act to “break up the monopolies” in healthcare as I testified last year in front of the @housebudgetGOP @HouseBudgetDems . We are on an unsustainable path that only helps shareholders but provides worse care at a higher cost. It’s time to put guardrails on private insurers, particularly for Medicare Advantage. Take those savings and put them back into the physician fee schedule and push physicians back into private practice. It will reduce the overall cost of care and increase quality.




0
0
0
Thank you Dr. Kamara for helping shine the light on the prior authorization issues we face for our patients. @bobjherman @statnews @politico @WSJhealth

Hey @Aetna @AetnaHelp Shared with patient permission We submitted prior authorization on 1/2 for a total knee replacement on 1/22 for a Aetna Medicare advantage patient. It was denied on Saturday 1/18 over the holiday weekend. Now your representatives are saying that since we didn’t appeal on Saturday, the surgery is denied and we need to restart the entire approval process. Additionally, no option was given to appeal the decision. We have spent 2+ hours talking to your staff with no recourse given. This is inappropriate. Saturday was a holiday weekend. The patient’s family took off work and flew in to support her during the surgery. The patient has failed multiple documented rounds of non-operative treatment, and has a successful knee replacement on her opposite leg. Her X-ray below clearly demonstrates bone on bone arthritis. This is a clear violation of Medicare guidelines. Another example of the need for the passage of S.4532 Improving Seniors’ Timely Access to Care Act @AAOS1 @AAHKS @CMSGov @cmaorg @HHSGov @MedicareGov @AmerMedicalAssn
#claimdenied #respectmyprescription
0
0
12
@levim195 Agree… it’s tough but I think we are striking the right balance and getting engagement across the board
0
0
0
I’m not sure I understand why we would fight to reduce anyone’s payments. There are reforms that will substantially improve pay across the board that should be considered. The G code (G2211) was a prime example of good intentions and horrible policy. We need to stop playing the medical hunger games and work to raise the tide for all boats.
0
0
0
I’m completely fine with what you are stating if that is how you feel. What we need is coordination in Washington. I have never worked with PPA, but if they have full time lobbyists and are working on healthcare, then I would love to ensure we are all communicating and working in the same direction with the same focus
0
1
0
And those organizations have had many wins over the years. Unfortunately moving a large ship takes time. We are making a difference but the systemic effects physicians are facing suggests we can no longer sit on the sidelines. I guess we should go back to the age old questions: 1) how many of you know your representatives 2) how many of your representatives know you The stories need to be told and the ideas conveyed but that takes a mix of national large scale efforts and then personal relationships with legislators. You have to have both. If doctors just write checks it doesn’t work. If they just show up once a year to DC or their state legislative house it doesn’t work. Today I see most doctors doing neither but then complaining about why they had to sell their practice, why their staff was reduced by a corporation, why they can’t start and own a hospital, etc…. To fix the problem we have to start becoming a part of the solution
2
1
13
Thanks for your post. I would encourage you to look at the Hassan Cassidy framework for site neutrality. They propose several different payment points and several different targets for site neutrality. Those choices dramatically impact savings. It will be interesting to see if Congress can coalesce around an agreement here. I would argue they are more likely to pay a rate that equals physician payments for outpatient work and equals ASC rates (not in-office rates) for procedures. There are wide reaching ramifications for each choice that need to be discussed in greater detail than can occur prior to reconciliation.
0
0
2
How? How can one defend their actions and simultaneously blame physicians for “charging too much”? Or are they just referring to hospitals? United has been an instigator and cause of massive consolidation. They are the largest employer of physicians. They have pushed doctors to employment. To the extent this is the hospitals’ fault, then what degree of responsibility do they take for continually putting their internal profits over sustaining the healthcare system? The irony here is that PBMs were found by the FTC to have profited billions of dollars the same week that they made this statement. United owns their PBM. The last year of articles has shown how United has used the Medicare Advantage program to extract billions of dollars through overcoding and cherry picking. Their own doctors have gone on the record about it. United is a massive part of the problem and pointing the finger is the wrong solution and is tone deaf. UnitedHealth defends business in wake of Thompson killing | STAT

3
8
52
RT @tylcole: @DrDiGiorgio I think a lot of docs and public don’t understand that the revenue streams have been intentionally diverted away…
0
34
0