

Dave Quirk
@2Quirk
Followers
1K
Following
578
Statuses
154
NWAS Clinical Support Manager & APP🚨| Developing pre-hospital clinical practice | Occasional lecturer | #RapidRecap 📚 | ...& away from work, the outdoors 🏔
North West, England
Joined October 2018
RT @2Quirk: 🚑🚨#RapidRecap, this time exploring Chronic Kidney Disease - a quick review of key points. Is it AKI? What's the difference? And…
0
11
0
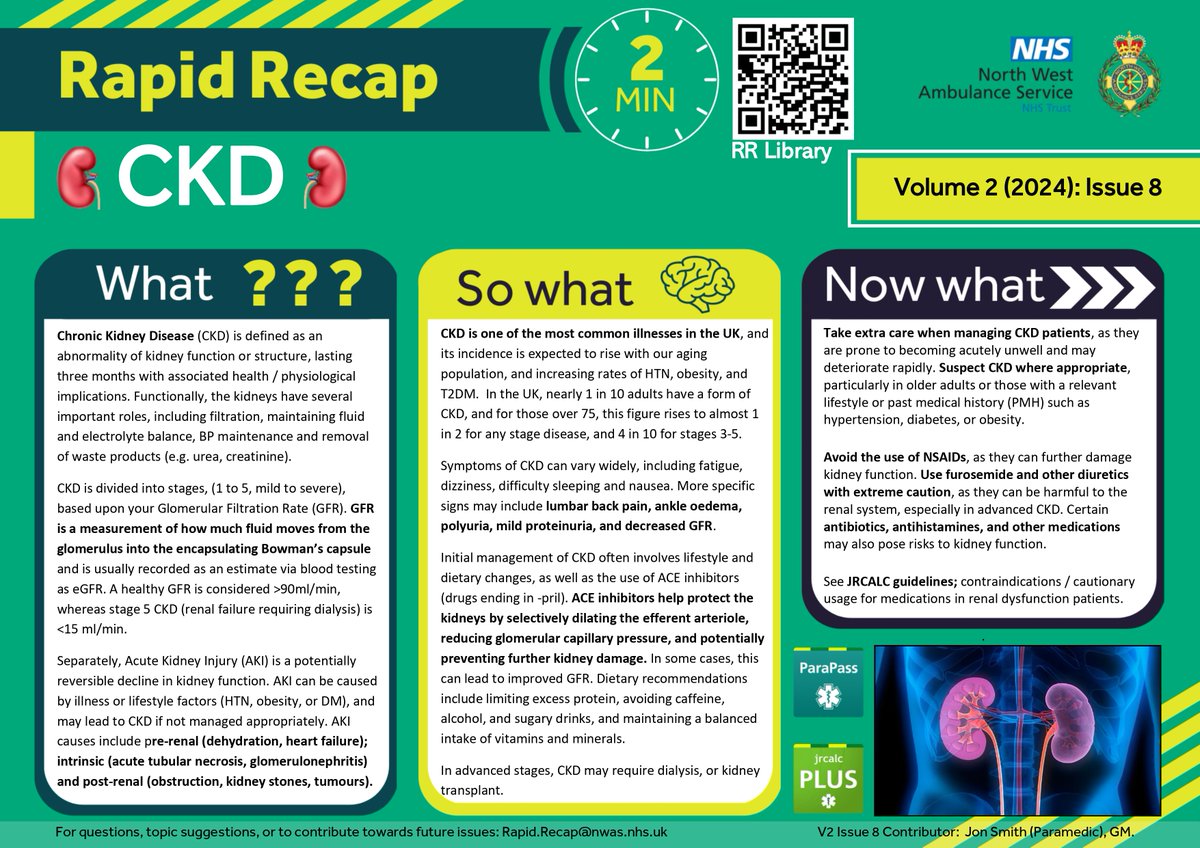
🚑🚨#RapidRecap, this time exploring Chronic Kidney Disease - a quick review of key points. Is it AKI? What's the difference? And what interventions should we be cautious of? See #JRCALC & #ParaPass for more... #studentparamedic #nurse #studentnurse #ambulance #FOAMed #paramedic
0
11
40
RT @2Quirk: 🚨🚑December's #RapidRecap looks at Psychogenic Non-Epileptic Seizures #PNES, helping us move past the historical pejorative term…
0
30
0
RT @2Quirk: 🚨🚑 In keeping with the pregnancy-related complications theme of our last #RapidRecap, this month, we explore bleeding🩸. Scan th…
0
28
0
RT @2Quirk: 🚑🚨🩸#RapidRecap: Sickle Cell Disease. It's most common in people of African or Caribbean origin; take two minutes to refresh und…
0
24
0
🚑🚨🩸#RapidRecap: Sickle Cell Disease. It's most common in people of African or Caribbean origin; take two minutes to refresh underpinning knowledge and recap the red flags 🩸🚨🚑 #paramedic #studentparamedic #nurse #studentnurse #ambulance #FOAMed

1
24
86
RT @2Quirk: ☀️🥵#RapidRecap -Heat illness 🥵☀️. Heat stress > heat exhaustion > heat stroke > mortality. Early consideration, recognition, an…
0
12
0
MSc ✅️....Tough, often overwhelming, yet achievable. A process made easier by having the right people around; a great cohort and top-tier study team.




8
0
113
See #JRCALC and #parapass for more info/guidance. And, have a listen to the brilliant @TheResusRoom podcast about heat illness
0
0
3
RT @NWAmb_Research: If you're a newly qualified or early career professional who has recently completed or are working towards your profess…
0
2
0


RT @2Quirk: 🚑🚨#RapidRecap STEMI. Early diagnosis and prompt transfer to PPCI are crucial. Minimising our on-scene time can positively influ…
0
31
0
@ParaAndy90 @h3l3na97 @RossM_2003 The most crucial factor is ensuring correct pad placement, that lateral pad especially⚡️
0
0
2
@h3l3na97 @RossM_2003 Defibrillators often increase joules for the first 3 shocks, 200, 300, 360... And the likelihood of reverting VF is highest at the point of arrest, then decreasing over time. Without stacked shocks, a 4-minute wait exists before 360j and there is also consequential chest trauma.
1
0
3
@RossM_2003 Definitely - it significantly improves defibrillation time and these patients are high risk of VF. From a human factors perspective, it keeps the clinician calm with good operating bandwidth as all they have to do is press shock 👌
0
0
3