
mandeep singh
@mandeep_mayo
Followers
7K
Following
6K
Media
688
Statuses
4K
Interventional cardiologist with passion for aging research. Proud dad and husband. All opinions my own.
Rochester, MN
Joined January 2020
Once you see it, you will never forget it. What is your diagnosis?

41
86
664
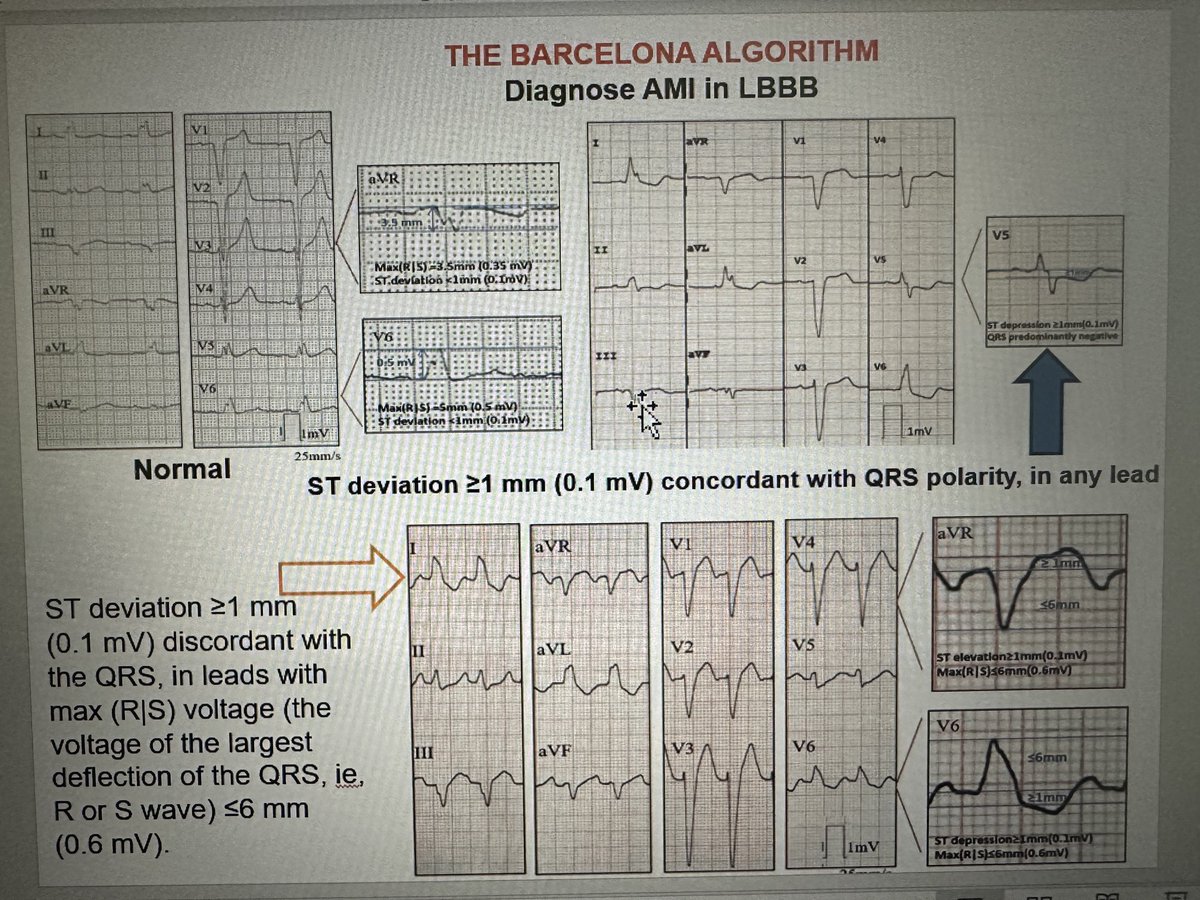
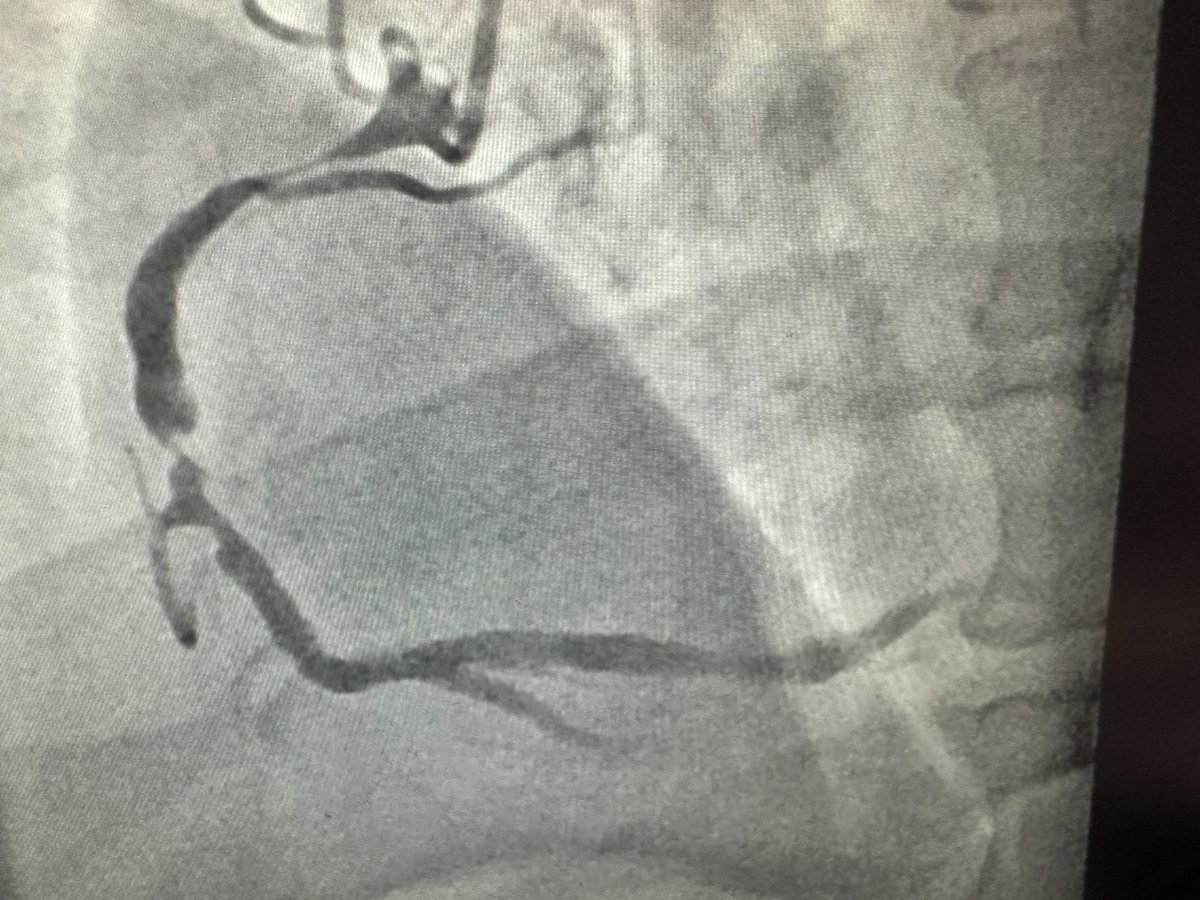
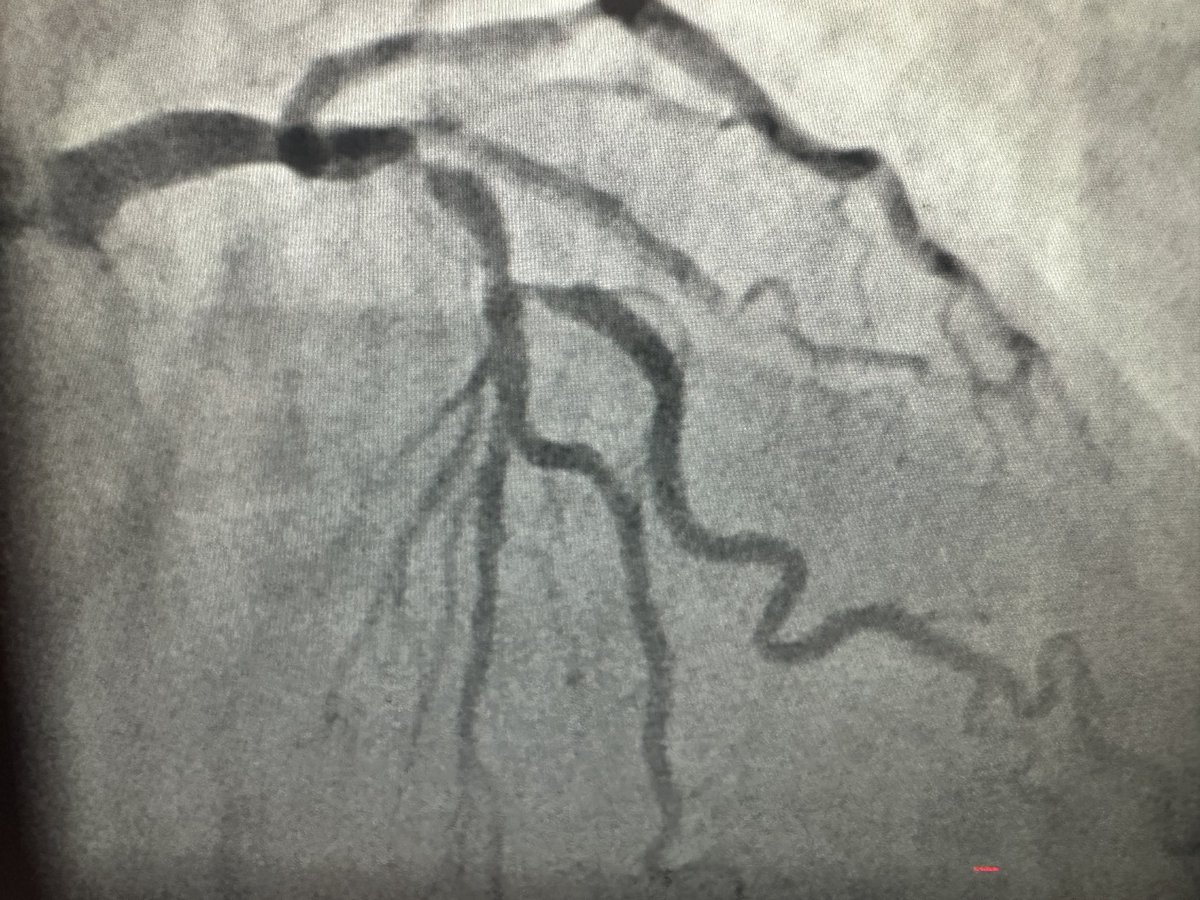
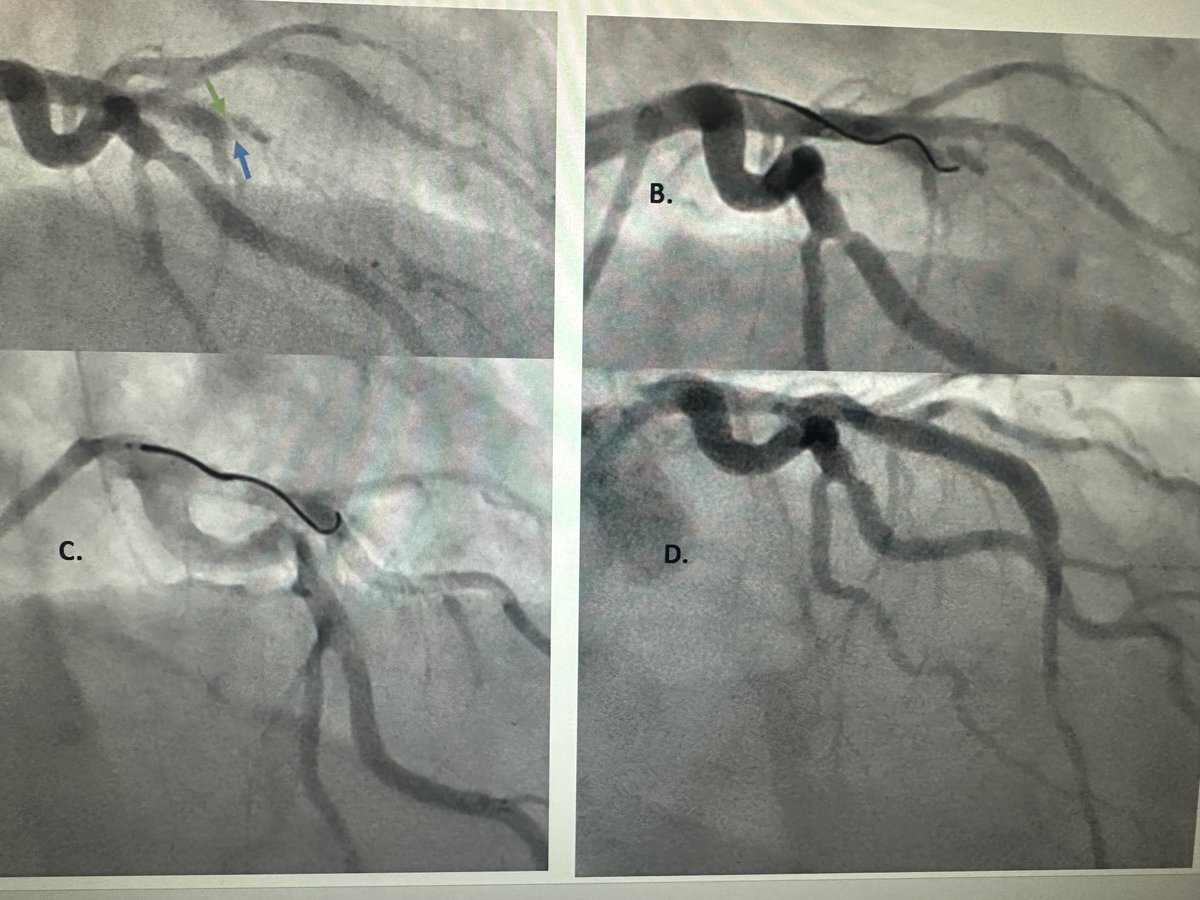
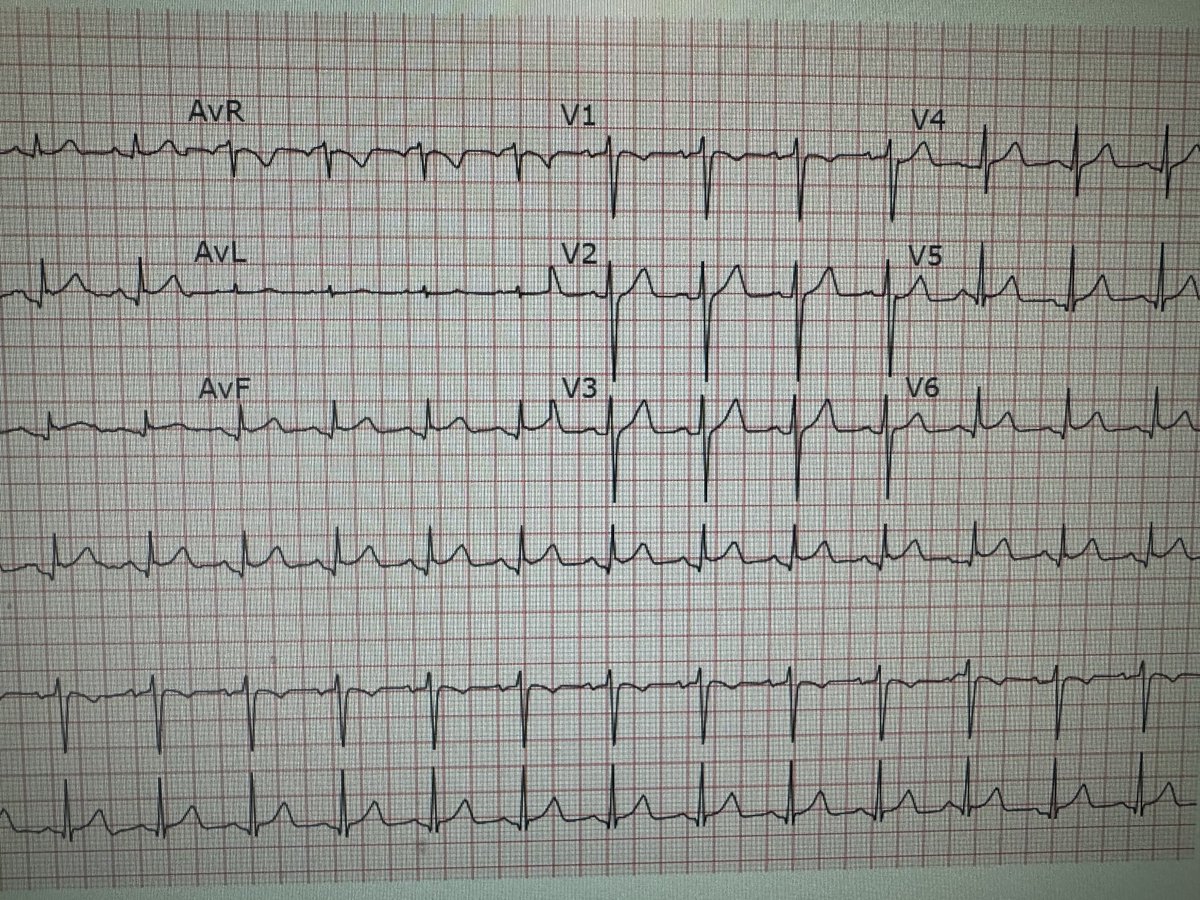
Out of hospital cardiac arrest. EKG done following resuscitation. What would you do next?

43
116
529
Sensitivity (36%) of the Sgarbossa criteria for AMI diagnosis in LBBB has been improved with Smith (91%) ST/S ratio <_-0.25 to now Barcelona (93-95%) with just 2 criteria. Just remember 1.concordant ST dev in any lead or 2. Discordant ST dev>1 mm in low voltage leads (R/S<6mm)
6
166
423


@FelixValencia10 I usually don’t give the answers so quickly but this is classic hypothermia with J or Osborne waves and normalized subsequently. Make a mental note, core temp<27F, found outdoors in MN winter; everything normalized with warming, normal echo
3
13
285
PCI for stable CAD needs to be revisited. The trials, COURAGE, BARI, ISCHEMIA are consistently negative when we compare ourselves with medical Rx. CAD subsets that need CABG, we lose again, SYNTAX (3VD/LM) FREEDOM (DM) NOBLE (LM), ?FAME3. What are we missing? Just do ACS-PCI??.
38
52
259


Please join me in congratulating my dear friend @adnanalkhouli in becoming the Associate Editor of JACC Interventions. What a proud moment for him and for all of us who work with him and his genius @MayoClinicCV!!.
39
9
224
Part 3:Coronary angio: . RAO Cranial .1. Separates septals from diagonals.2. Useful for alcohol septal ablation in HCM.3. PCI of mid/distal LAD.4. Types of LAD: A-C: Ends before apex (A)-wrap around (C).5. Divides LAD: Proximal (before 1st septal),mid (between 2 diagonals)&distal

2
33
209
Part 2 for fellows:. Coronary angiography in LAO cranial view. ⬆️radiation dose to operators. Very good option to. 1. Outline mid & distal LAD lesions. 2. Ostial LM disease (LM stent placement).3. Left dominance: (LPDA from LCX)

2
40
180


@DrSiyabMD The proudest moment for any parent would be to see his/her kid follow their footsteps and you have just done that. Congratulations 🍾 to you both and may you pass the baton to your kid!.
3
7
163
90 YF, severe PAD and Sx AS. Transfemoral TAVR with shockwave assisted sheath placement. See what happens and I will share what we did.
23
15
170
For fellows:. Angiographic underpinnings to explain why AV nodal blocks are much more common than SA blocks in inferior STEMI. Location of inferior STEMI before RV branch associated with STE in V3 and V4R, poor prognosis and possible shock.

1
41
167
From my archives: what would you do next and what would you NOT do?

47
33
164
I believe in #safe vascular access rather than radial first or safe femoral. Patient’s safety is the only thing that should matter. I tried most of the tricks without success to engage LM. I usually follow “<5 min rule” to switch from radial to femoral.
14
7
155
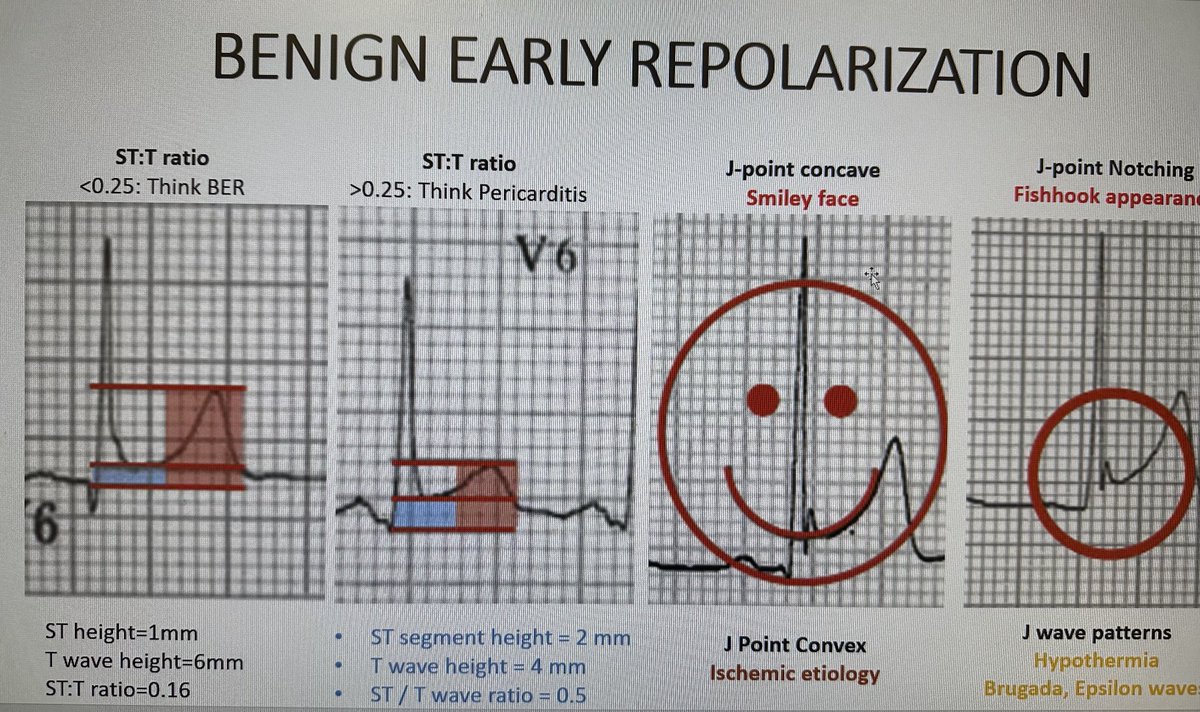
BER vs. Acute Pericarditis: Remember the setting (ASx vs. Sx) and T wave height in precordial leads (higher in BER) with resultant smaller ST/T wave ratio.

2
37
153
Rules of left main engagement: 1. Always look at the pressure before injecting. 2. Pull the catheter to align, give NTG. 3. If still damps, take smaller French (5F to 4F). 4. do a non selective injection. 5. If can’t see, do RCA injection, it may fill the left system.
6
34
153
If you can ask one question or do one test on this patient with cardiac arrest, what would it be? Look at the angiogram and the EKG very carefully.
63
19
146
Starting 2024, am teaming with my colleague @abhishek_mbbs to deliver once-a-week EKG tutorials. Together we will cover the breadth of EKG abnormalities. I will cover AMI complications & EKG with unique clinical conditions. Dr Deshmukh will cover rhythms and heart blocks.
2
14
141
Two catheters: Two tracings- Same patient (Circulation 2012)

2
23
125
Patient was taken to the Cath lab. Hemodynamic assessment is usually not required to make the diagnosis of constriction; symptoms and echo suffice. What is your diagnosis based on the following tracing?

11
19
126
Part 4: Coronary angio: RAO Caudal. 1. For LM, prox LAD & LCX lesions. 2. Outlines left AV groove (MAC, coronary sinus, MV).3. Course of anomalous coronaries. 4. Proximal (before) and distal LCX after OM1.

1
16
125
Teaching points: 1. No more injection. 2. Cover ostium (IVUS+). 3. Surgery rarely needed (complete resolution of dissection). 4. Surgery needed if >4cm, pericardial involvement or AI. 5. Repeat imaging to demonstrate resolution



4
22
123
Part 1: Coronary angiography for fellows: LAO caudal view. Orient yourself to the layout of coronary arteries in relation to LV & LA. Used for detection of disease in LM, proximal LAD and proximal LCX.

2
19
122
STRETCH Trial: stretches can improve pain during interventional procedures. Improve your ergonomic health by doing 15 mins of daily stretches. Our research published in @MyJSCAI @BrendenIngraham @rajivxgulati @pattypellikka

4
42
121
Interventionalists are:.🟢MADE 🔴May be destined 🟣 But NOT BORN. So work hard to become one!.
2
11
118

Five diseases should never leave your thoughts when you see a patient with chest pain or shortness of breath. 🧿Aortic dissection.🧿Acute myocardial infarction .🧿Pulmonary embolism.🧿Amyloid heart disease.🧿Constrictive pericarditis.
8
17
113
Shortness of breath in a 68ym with prior cardiac treatment. What is your diagnosis?
22
21
109
Part 5a for fellows: Graft angiography. All you need to know about LIMA

2
20
109
Part 9: Aorto-ostial disease for fellows. Geographical miss, damping, and inadequate expansion of stents are the main challenges. Here are my 10 tips to avoid problems during diagnostic angiogram and PCI.

3
29
110
Five “G”eneral principles of successful PCI:.1. Good guide support.2. Good view(2 lumens (A), lower is false (B), aimed for upper. 3. Good angulations @ wire tip ( primary & secondary bends) & with MC (Twin pass or angled MC: used).4: Good friend@benhibbertMDPhD .5: God
5
21
105
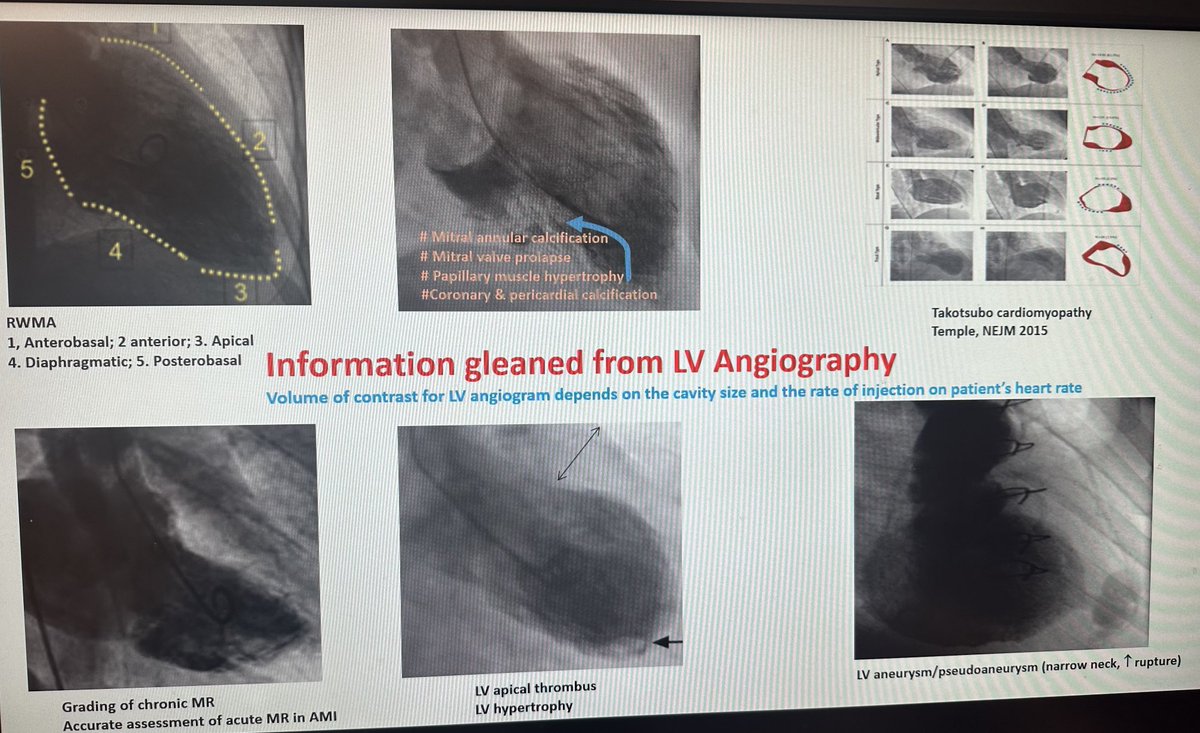
70+ M with chest pain. LV angio shown, what is your next step?
13
16
99
BER: Final frontier. Stable, STE (concave upwards, precordial) in young males, may disappear with older age, more prominent at slower heart rates. T waves prominent with resultant low ST:T ratio.
1
21
97
ACS presentation. Unable to pass any thrombectomy device. What would you do next and what do you anticipate?
31
15
94
What is your diagnosis in this women in 70s, nulligravida and height 144 cm. Presentation with hypertension and CHF.

21
19
97
Big shoutout to @rajivxgulati for becoming our next Cath lab director. He is a dear friend and a great colleague 👍👍.
17
9
97
This was the CXR that started it all. What pertinent history you will take from this patient?

19
17
94
Separate coronary Ostia. 1: For LAD use a shorter curve or CCW your catheter to engage. Or push your XB from the aortic root. 2: Bigger curve for LCX or CW rotation will engage the LCX.
10
26
96

DAPT preRx not indicated unless STEMI/coronary anatomy is known. Reasons:.1. Can’t predict LM/3VD. 2. If LM/3VD, CABG is delayed.3. ⬆️ bleeding with no ischemic benefit (ACCOAST, SCAAR, ISAR-REACT-5, DUBIOUS trials). 4. Stent thrombosis risk <.5%.5. European guidelines Class III.
7
23
94
There are 5 areas where PCI couldn’t make meaningful inroads:.1. CTO-PCI: no improvement in survival, LV fxn, even sx?. Reserved for highly symptomatic pts. 2. SIHD vs medical Rx: a struggle .3. Survival improvement in SIHD.4. Late revascularization in STEMI .5. Prevention of AKI.
8
17
91
FOR FELLOWS . LV angiography is a very useful tool that everyone should familiarize with. Here is all the information that can be obtained from this simple test.
4
22
92
Don’t ignore high and rising troponin in older adults with atypical symptoms. How would you approach this?
34
12
91
What is the ONE question you will ask this patient to come to the right diagnosis?
33
11
89
Fascinating case! Your approach. 1. Guide catheter and wire. 2. Stent size and length. 3. Anticipate which complications
21
16
90
This is what we did. Valve was free on catheter, Inflated the balloon but unable to bring stent valve down to descending aorta due to Ca2+. Deployed 1st valve in ascending aorta using a 28mm balloon (30mm aorta) for a 23mm valve and then deployed 2nd valve. Pt. Discharged day 4.
7
14
91
Be careful with non-coaxial AL guides with proximal lesions, especially when the pressure is damped as this can result in extensive iatrogenic dissection.
9
14
89
Interventional successes of the past decade:.1. TAVR (low, intermediate, high risk, PARTNER & Evolut).2. Radial access (MATRIX).3. IV imaging ( RENOVATE COMPLEX PCI).4. ⬇️ stent thrombosis with Everolimus/Zatrolimus-eluting stents. 5. Shorten DAPT duration (MASTER DAPT/TWILIGHT).
0
25
85
Catheter-directed lysis followed by thrombectomy with Export catheter, 5mm DES stent. Distal embolization dottered with a balloon. Acute stent thrombosis the next day.
25
18
89
What would you do? Male in 50’s with off and on chest pain for a week, worse hours before presentation. Smoker and has diabetes mellitus. Hemodynamics stable.

31
13
86
PVCs noted during PCI are not benign. Below are some of the causes. 1. Reperfusion arrhythmias. 2. Catheter damping. 3. Perforation (wire/large vessel). 4. Flush is left on. 5. Distal embolization of thrombus. 6. No reflow.
6
16
88
LM engagement: would you go up or down on the curve of this 3.5XB guide? Would you rather use another guide? Even after 30 years in practice, this confusion crops up!
50
16
85
If you are allowed one question to ask this patient, what would it be?

50
9
84
If STE (EKG 1) reverses (EKG 2) and chest pain resolves within minutes: 1. How would classify the ACS? 2. Would you take the patient to the Cath lab right away/wait. 3. Would you give lytics. 4. Can this be Printzmetal angina?


39
17
82
3 musts in all pts with STE. 1. Check all pulses vascular deficit indicates ascending aortic dissection. 2. Put stethoscope on precordium & lungs for VSD/MR/S3/crackles. 3. POCUS if available for RWM (location of infarct) LVFxn & pericardial effusion (FWR). Our pt had dissection.

1
14
84
Severe, accidental hypothermia (core temp in 70s). Causes of VF with heart blocks/Brady (1. Hypothermia {Osborne, prolonged RR, PR, QT} 2. K^ 3. Hypothyroid 4. Hypopituitary. 5. Myocardial {amyloid, sarcoid} 6. Dig toxicity 7. Brady-VF. Congrats everyone who guessed right!
7
10
86
Not all perforations are created equal: Stent perforations happen due to high pressure (22atm) in a calcified lesion with an underexpanded stent. How would you manage this one?
25
24
83
Complications of right and left heart catheterization. Numbers to remember to take informed consent!
1
16
83
This was Type I perforation (Ellis Classification) successfully stented with no clinical sequelae.

2
17
85
Teaching points.1: use aggressive guides (AL/IK).2: use GCE.3: use hydrophilic wires/Pilot with MC.4: try 🎈1st, if unable atherectomy .5: IVUS only if you can.6: stent normal-normal segment.7. Stent size to normal not ectatic seg.8: beware of concertina, perf, dissection,malapp
8
12
82
2/3: we ended with no reflow after 🎈 and 4.0*32 DES. ACT>280s. BP:80mmHg; EKG: STE. Next step??
41
17
79
FOOD FOR THOUGHT: PCI before TAVR needs to be revisited & purpose redefined. Not sure PCI improve TAVR outcomes. When was the last time, one saw plaque rupture of untreated lesion. Barring ostial dx, we need to be conservative. Presence of angina shouldn’t be the driver for PCI.
14
9
80
How would you manage? H/o stent in LAD, no fever or endocarditis!
31
10
77
Iatrogenic coronary dissection. How would you approach? Share your tips and tricks. Patients started to note chest pain!
23
15
80
Keep this diagnosis in your memory bank. Excellent CT-Angio correlation and surgical cure of angina in this young patient.
11
14
79
Coronary dissection management depends upon patient’s hemodynamics, dissection type & if wire across is present. If wire position is lost, use multiple wires to find the true lumen aided by IVUS. @PurumittalDr @benhibbertMDPhD Ben has published the largest series



3
16
79
66-YM presented with prolonged ischemic chest pain to your ED. The pain started 35 minutes ago. What is your next step?

18
16
78
How would you wire the LAD & Rx the bifurcation with diagonal branch?

13
9
77
90 year old presented with anterolateral STEMI. Pictures shown. Wire went in with some manipulation. Took the first shot after PTCA, patient had VT. What is your diagnosis and what would you do next?
26
20
77
STEMI call was activated on this young smoker presenting with chest pain. What would you do next?
49
15
74
Thanks everyone for their input. We couldn’t cross with just a wire (Scion black & Whisper). Used supercross 90& 120 without success. Used Twinpass, retrograde wire approach with a secondary bend on a Whisper. Wires on deck: Pilot50&FielderXT. Procedure on deck: atherectomy
11
7
72
This is what we all live to do- Save one life at a time. Performed PCI of LAD and RCA. With ongoing CPRTough to cross CX:CTO. Tried micro catheter-supported wire escalation. Pt recovered, will be dx, EF 47%. No rib #. Doing well. Thx to anesthesia, RN, techs for saving his life .
8
3
75
It is wrong on multiple fronts! Please abstain from such practices.

13
11
77
Pre-op angiogram. Can you guess which cardiac surgery other than CABG?
20
13
74
Part 11 for fellows.Calcified lesions in PCI. Here are 2 slides that encapsulate the contemporary management strategies. Important to evaluate the degree, extent, and depth of Ca2+ involvement for optimal results.


1
26
75
Young MI Recap: commonest cause is plaque rupture. If total occlusion with thrombus seen on CTA it is NOT SCAD. Do angio on every suspected SCAD.
3
14
74
Your diagnosis and management of this young male, smoker, Cholesterol over 300, LDL>200,TG >300.
19
10
69
Identify everything in this video and win accolades from your peers.
8
15
73
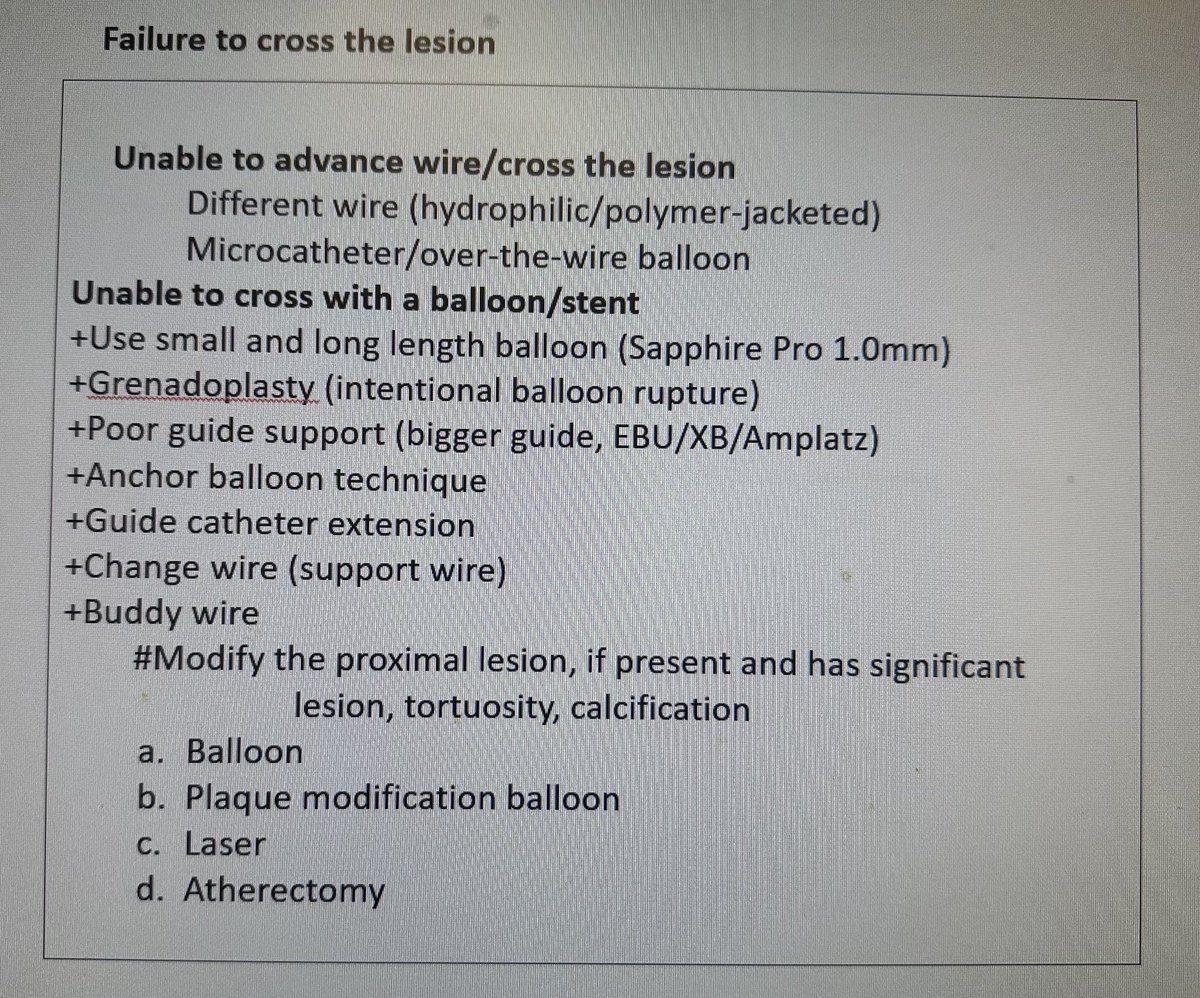
My summary slide. Helpful management tips for inability to cross.
4
16
73
What is one test you should always review before a routine right heart Cath?.
34
5
69
Eosinophilic myocarditis with extensive myocardial thrombi and poor biventricular ejection fraction.
5
13
70
IVL is not benign. This was the MAUDE presented as an abstract last year. Coronary perforations & dissections are common. Be careful in eccentric, calcified lesions and in post dilating at high pressures with NC 🎈as calcium nodules/eccentric Ca2+ may have been adversely modified

6
12
70
During a heart catheterization, this was detected? Your diagnosis!!

18
7
71
Our patient severe coronary vasospasm induced by IC Acetylcholine
2
10
69
Your approach in this ~90ym NSTEMI.1. Beta blockers & nitrates.2. CABG.3. PCI
26
5
70
Be vigilant: what is going on here during a coronary angiogram?

34
8
69
1. Sx (chest pain, syncope, F/H) differentiate early repol pattern (EP) from synd (EPS). 2. ER typically refers to J point⬆️.3. Young 👨🏼🏫, f/h of SCD or h/o syncope.4. STE in inf leads, >J point elevation, ⬆️J amplitude ⬆️arrhythmia risk.5. ⬇️/➡️ST after J wave has ⬆️VT risk

0
17
69