

Iain Beardsell
@docib
Followers
9,755
Following
377
Media
1,847
Statuses
14,229
Consultant in Emergency Medicine and Associate Clinical Sub Dean @UHSFT . Honorary Principal Teaching Fellow @UoS_Medicine . @stemlyns #FOAMed
Wiltshire
Joined August 2009
Don't wanna be here?
Send us removal request.
Explore trending content on Musk Viewer
Maggie Smith
• 785844 Tweets
Netanyahu
• 622037 Tweets
Beirut
• 486962 Tweets
القادسية
• 423643 Tweets
Nasrallah
• 306100 Tweets
Zelensky
• 262196 Tweets
Harry Potter
• 211815 Tweets
Lali
• 201017 Tweets
بيروت
• 163760 Tweets
الزمالك
• 120127 Tweets
Acapulco
• 95699 Tweets
#الضاحيه_الجنوبيه
• 79155 Tweets
I-40
• 73039 Tweets
マクゴナガル先生
• 54231 Tweets
حامد
• 35722 Tweets
Van Gogh
• 29508 Tweets
Willie
• 27821 Tweets
Asheville
• 26536 Tweets
FONDEN
• 25808 Tweets
#حسن_نصر_الشيطان
• 18311 Tweets
Dortmund
• 15527 Tweets
Barcola
• 15406 Tweets
#السوبر_الافريقي
• 13565 Tweets
Bane
• 12104 Tweets


















I very, very rarely swear on here, but Lawrence Fox is a colossal twat isn’t he?
105
57
2K
I have been a doctor in emergency (A&E) medicine since 1999 (before the four hour target) and I can honestly say it has never been as bad as it is today. Right now. I have no idea how the clinicians, nurse and others will keep going to work everyday.
38
383
2K
Evening Abby. Finally a question I can answer! There are many causes of a tachycardia. Sometimes it’s just a physiological response to the body needing more oxygen in the tissues, but it could also be an arrhythmia like fast AF or even VT. I hope that helps. Yours aye. Iain.
23
141
1K
Hi Abby. It’s really kind of you to show such an interest. I think it’s probably getting an arterial line in under ultrasound guidance in a patient with no palpable pulse. There’s nothing like it. All best. Iain.
43
74
1K
The uncomfortable truth that dare not be said is that many do not need to see a GP or attend A&E. Society is now about the individual not the whole. We’ve seen it for years- “so what if there’s dying people in Resus? What about my sprained ankle?”.
49
119
1K
When you attend an A&E/Emergency Department.
1️⃣ We will see people in order of clinical urgency.
2️⃣Arriving by ambulance does not mean you will be seen quicker
23
221
985
Just for fun I asked our night team of doctors how many had been Head Boy/Girl at school. Over 50%. Sometimes we forget just how high achieving our colleagues are. They are (literally) the academic top 1%. We need to empower them, not patronise them in their roles.
74
45
977
I notice the
#JuniorDoctorsStrike
has dropped off the
@BBCNews
website front page and isn’t even the top health story. Press coverage often negative and patients undeterred from attending A&E. I fear HMG has no reason to negotiate. What’s the
@TheBMA
next move?
32
140
758
He’s a farmer in A&E. Immediately refer to ITU.

A 29-year-old farmer presents to your local ED with a bite mark over the upper left calf 🕷️ He is physiologically stable with a NEWS of 0.
How do you manage this case?
🆓
#FOAMed
➡️
@HassanNassar90

8
5
23
17
15
611
It is time for a national discussion about what it is reasonable to expect for emergency medical care from
#NHS
. We can no longer just see everybody and anyone who turns up at A&Es’ doors. It is just not possible. We have to be there for the acutely unwell and injured.
33
112
589
Never underestimate the toll it takes on you walking into a hospital every day. Surrounded by the sick, injured and sad it’s hard to remember that the whole world isn’t like that. I genuinely don’t think the public (or politicians) have any understanding of how hard it can be.
18
63
574
I have a confession to make. Please don’t judge me or think me less of a man or clinician.
I really don’t mind when people call it ‘A&E’…
46
7
515


There seems to be an awful lot of pressure to “live your best life”. Some days I’m content just to live an average life: pottering along; trying not to shout at my children too much; eating only 2 of my 5 a day and letting the world pass me by. And not to feel too guilty about it
15
56
460
I work in an A&E/Emergency Department.
I do not work on the “front line”.
I’m not a solider in battle.
16
24
446
The bit I don’t understand is why no one telling the public that their expectations of the
#NHS
are simply too high. There needs to be an element of self care first for many. GP appointments are available, as are A&E services, but we cannot cater for the worried well.
39
38
441
I wonder of headline should actually be
‘Consultants standard hourly pay is less than almost any tradesperson who might work on your car, plumbing, tax return, divorce or house renovation’.

9
70
420

We often hear grand plans for A&E restructuring, but what small things would make your ED more efficient?
I’ll start...
*Printers that always work
*Not having to sign ECGs/VBGs for patients who didn’t need them in the first place
*An up to date contact list
Your turn....
89
33
394
Is the sunflower lanyard now the 21st Century version of the soft cervical collar?
12
21
361
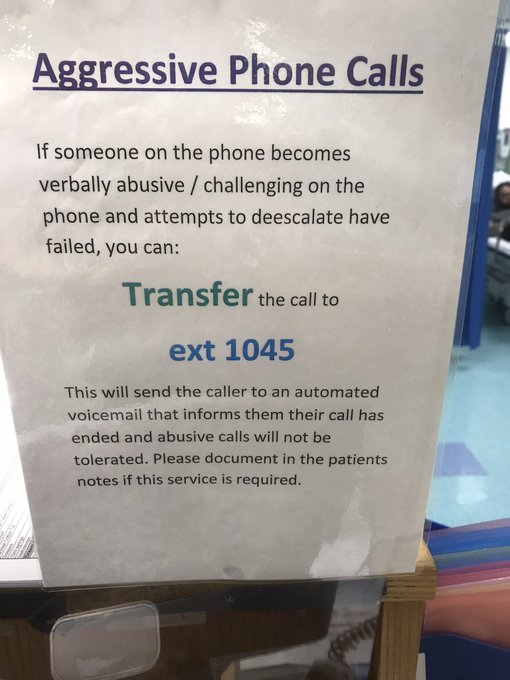
@zackferguson
We now have this. The recorded message is brilliantly blunt and then cuts the caller off.
17
47
352
“The A&E target” and thoughts about why we’re struggling to meet it. A thread👇
27
211
342
Working in A&E over the next few months will be challenging, but I can’t be the only one who thinks it’ll all pale into insignificance compared to the night the lockdown ends....
10
28
346
The ED consultant when one of the inpatient teams is giving an ED junior doctor grief about a referral....
6
49
342
Only because you’re too young to remember ‘Sleek’. The Godfather of all tapes.

Which is your favorite medical tape and why is it Transpore?

218
1K
9K
55
8
335
I’d go with “no”, “no” and “no”. The future in the UK is chronic pain, psychiatry and geriatrics.

Do you believe ultrasound is the future of Emergency Medicine?
Do you believe video laryngoscopy is the future of Emergency Medicine?
Do you believe HEMS is the future of Emergency Medicine?
Some of the questions posed by
@davidstantonza
at
#badEM19

4
8
32
17
59
318
🔟Being in a hospital does not make you immune from common courtesy or the law. If you abuse us physically or verbally we will call the police.
I’m sure colleagues may want to add to the list…
8
21
320
Should “Advanced Life Support” be renamed “Basic Life Support Plus”? Resuscitation has moved on past generic algorithms. ALS really isn’t advanced at all, but gives the impression to providers that it’s the standard to aspire to. And those going “beyond the manual” are rogue.
40
46
303

We often talk about flow out of the Emergency Department (A&E) but is it time to have a serious discussion about who gets in at the front door? The system simply isn’t capable of looking after the entire population’s range of health concerns. Do we need to redefine ‘emergency’.
66
35
308
A very senior surgical colleague once said to me ‘I have no idea why we expect you to make a diagnosis in four hours. After several days and multiple tests I often still don’t know what’s wrong’.

7
31
300
Those in healthcare aren’t leaving because they don’t want to make sick people better, they’re leaving because of the public demand to tell well people they’re not sick.
6
24
287
Until we all acknowledge that the ED/A&E doesn’t have endless capacity, that corridor care is unacceptable and that the risk must be shared across the whole healthcare system nothing will ever change. I’m tired of inpatient teams using “but we’ve no beds” as an excuse.
13
83
285
Dear Junior Doctors. Next time a consultant questions why you ordered a CRP/D-Dimer/CT/ just reply by simply saying
“an abundance of caution”
4
17
284
Yes children, phones used to look like this, were attached to a socket and (best of all) when we answered we repeated our own telephone number. Yes. We repeated our own phone number (I can still remember ours from 40 years ago).

87
22
282
A patient with known advanced cancer shouldn’t be in an A&E at all. They should be directly admitted to an oncology or palliative care ward. This misuse and misunderstanding of what “A&E” is for is a major part of the problem.

Jeremy Corbyn tells ITV debate a friend with advanced cancer had to wait 8 hours in A&E for urgent treatment - staff under too much pressure
0
1
6
25
46
277
We’d never assume teachers would be able to be doctors without years of training, so why do we assume doctors can be teachers?...
26
42
277
5️⃣ Clinicians in A&E are specialists, but in the management of emergencies. We are no good at rashes, chronic illness and other medical problems that have been going on for more than a few days.
6️⃣ We are not a substitute for ‘I don’t have a GP’
5
27
281
As I am sure many medics have, I had an email from a national newspaper today asking me to comment on the current state of emergency care. I redirected them to the
@RCollEM
Communications Dept who are doing an excellent job. Important we have a single strong voice.
3
32
278
Honestly. If he can’t get an increased care package to keep him at home what hope have the rest of us got?
Prince Philip taken to hospital as a 'precautionary measure'

11
44
267
Hypoxic drive as the cause of rising CO2 in COPD is a myth. Please can we stop teaching this?

16
92
264
A quick guide to how Consultants in the
#NHS
are paid (as this may be a hot topic over coming weeks).
The basic unit of pay is a ‘PA’ or programmed activity. In ‘normal hours’ a PA is four hours. A full time contract is 10 PAs (40 ‘normal’ hours per week). 1/10
12
63
261
Good question Katie. I’m no cardiologist, but it would usually be via your femoral or radial artery as far as I know. Although, of course, in an emergency a clamshell thoracotomy would work too. Enjoy your dinner. Iain.
8
44
248
As Trusts seem to be competing to outdo each other on the quality of their “goody bags” at
#induction
, I can’t help but feel most starting new posts would swop it all for a (decent) rota in advance, no pointless stat and mand, access to parking, a commited Ed Sup and a pay cheque
12
33
245
Just my occasional reminder that being a Clinical Lead in a specialty in an
#NHS
Trust is an almost impossible job. Trade Union leader and Line Manager. Two masters with often very different needs and you’re stuck in the middle. Did it for three years: it almost killed me.
28
17
242

7️⃣ We are not a substitute for ‘my GP doesn’t take my problem seriously’ (which, by the way we don’t believe).
8️⃣We cannot get your out patient appointment brought forward.
9️⃣ Shouting at us doesn’t make us want to help you
10
16
235
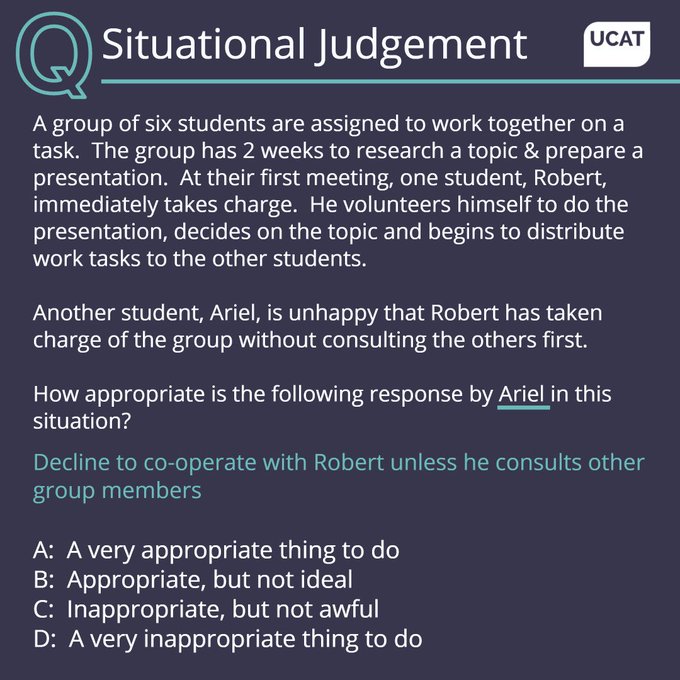
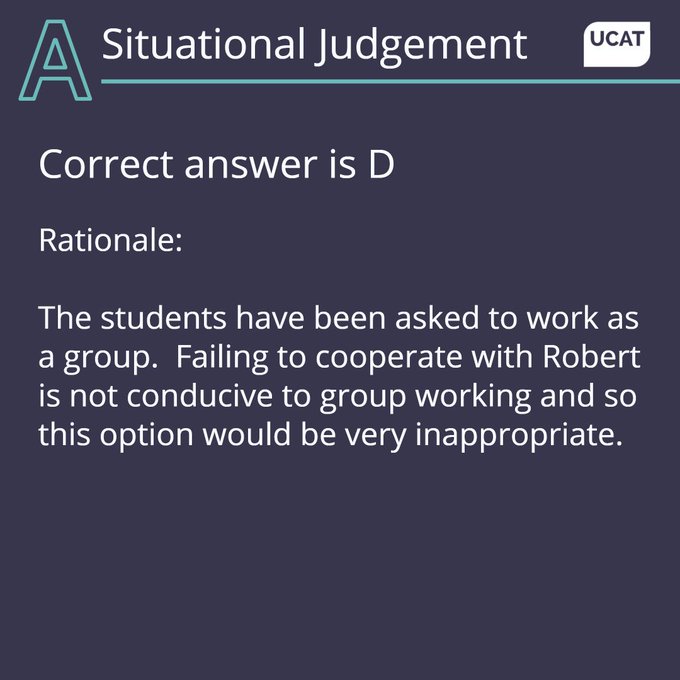
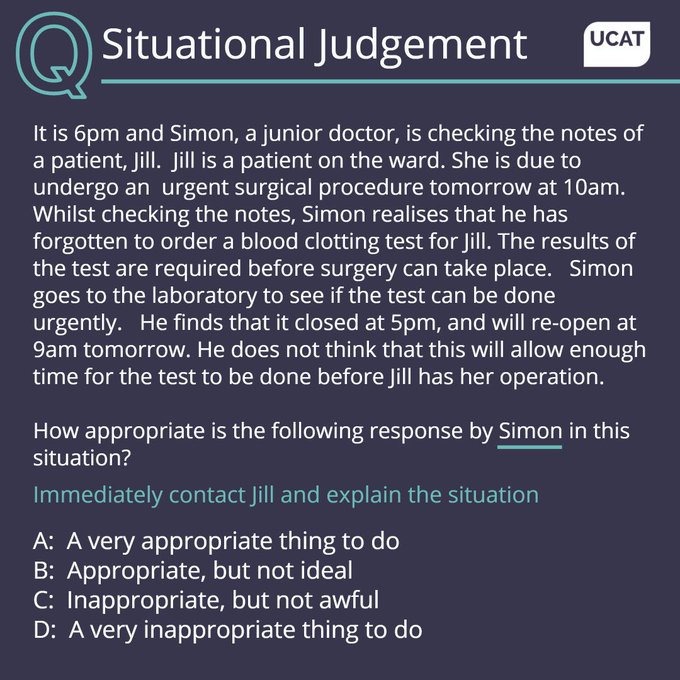
Our next
@UCATofficial
question.
Personally I think Ariel is pretty brave to stand up to Robert. All too often medics stand by and let bad behaviour happen. Ariel isn’t doing this and fair play to them. I’d answer A. (Robert is just the sort of person you’d dread working with).
81
16
231
Gosh Katie, I’m surprised I’m opening up to you so soon after meeting, but I’d say spending 10 years trying to tweet someone funny, only for someone else to post the exact same thing 12 hours later and getting 21 thousand more likes than me. At least I was his “inspiration”. Iain

10
9
229
I’m starting a crusade that not every patient attending the Emergency Department needs a venous blood gas and an ECG. Who’s with me?…
28
9
225
Just in case you're missing
#smaccDUB
(or want to know why thrombolysing submassive PE might be a bad idea).....

14
140
220
Controversial opinion- higher specialist training should be good enough that the ‘Life Support’ courses are unnecessary.

I currently can’t afford the £1000 for APLS and NLS, but need to put it on a credit card. 18% APR for the next 5 months, which isn’t insignificant. Doesn’t seem like anyone cares about this?
50
48
305
18
12
216
Saddened to hear one of our very promising FY2s has withdrawn from their place on the GP training scheme for next year. His future is now uncertain, but he said he simply ‘can’t see myself doing that job’. Urgent action is needed.
12
34
215
I have decided that it’s misleading for patients when surgeons use the prefix Mr/Mrs/Miss/Ms after passing an exam. Much better if they use Dr Their Name FRCS. Otherwise patients might think they are not seeing a real doctor.
52
18
212
I realise I really shouldn’t say this, but I can’t stand the word ‘resilience’....
23
10
203
Here’s an idea- for 24 hours why don’t as many people as possible post their positive experiences of working and training in Emergency Medicine. It doesn’t have to be monumental, just the little things that make it all worthwhile.
59
33
200
After some reflection I have concluded that Emergency Care in the UK has never before been under the constant, unrelenting pressure as it is now. Every shift feels like a struggle (and I’ve been doing it a while). How do you keep yourself positive on shift (and after)?
25
31
195
We’ve been trialling a new way of ‘front door’ working this week at
@UHSFT
. My biggest take home-we need the most senior decision makers possible available as early as possible. This may make some uncomfortable and echoes of ‘that’s not in my job plan’ will bounce off the walls…
30
25
193
I defy any Emergency Physician not to get anxious watching this. And then to resist telling a trampoline horror story to an unsuspecting passer by.
17
27
193
Most blood tests (and chest X-rays) performed in the emergency department are completely unnecessary.

🙋♂️ What’s your unpopular opinion in medicine that will get you in this position?
#MedTwitter

175
41
207
24
12
197
When, as trauma team leader, you suggest to the newly ATLS certified registrar that the haemodynamically normal trauma patient with an isolated limb injury only needs one cannula.
7
25
194
3️⃣Our clinicians each see on average one patient an hour. If there are 70 patients waiting to be seen when you arrive and there are 10 clinicians, and your problem is not urgent your wait will be at least 7 hours.
4️⃣ More tests does not mean better care. Perhaps even the opposite
3
12
196
When my children are taking ages to get ready for school I follow them round the house with a clipboard yelling “you’re going to breach”...

How has medical parlance made its way into your everyday language?
I'll start: I say that things have "nadired" (verb) all the time, and that it's "not unreasonable" to do a given thing.
Ex: My mood had nadired, so it seemed not unreasonable to eat an entire box of Oreos.
183
67
1K
5
24
197
A very senior surgical colleague of mine once said ‘I don’t know why we expect you to make a diagnosis in four hours, when often, after they’ve been an inpatient with us for two days I still don’t know what’s wrong with them…’

Would be interested to know the thoughts of UK surgeons on this, particularly those who don’t think surgery should be taking referrals from ED without a confirmed surgical diagnosis
@MStott88
?
11
4
53
9
19
193
Well Katie, a combination of:
Zygomaticus major and minor: Pulls up the corners of your mouth.
Orbicularis oculi: Causes the eye crinkle.
Levator labii superioris: Pulls up the corner of lip and nose.
Levator anguli oris: Raises the angle of mouth.
And a few others. Iain.
4
21
191
Having high blood pressure with no symptoms is not a medical emergency. It’s a risk factor for future disease. Yes it needs attention, but only in the same way smoking cessation does. And for many the first step isn’t tablets…
14
22
184
Please only go to A&E if you have a genuine medical need.
It's nothing to do with the cyber attack, just general advice.....
3
112
184
Thought this question and answer from
@UCATofficial
was really interesting. As a consultant I definitely wouldn’t have answered D. Junior doctors are highly trained professionals. Simon sounds like a conscientious doctor, making a patient centred decision.

55
11
181
Two very simple words, uttered by both patients and staff, have crippled healthcare.
“What if?....”
This has lead to increased attendances, increased length of stay and overinvestigation. I fear this can never be reversed. We seem incapable to accept any risk however small.
18
64
181

I swear to God if he visits Salisbury Cathedral I’m going to lose my ****. To be near such medical superstardom is overwhelming…


6
3
177
I’m a complete devotee of the original Morse books (and TV) but having just binge watched the latest series there’s a chance I like
@EndeavourTV
even more. Beautifully played by all involved.

7
5
169
Yes there’s an aging population and COVID, but do we really believe that public health is worse now than two decades ago? Phone consultations work because it is a trained person absolving the individual of the responsibility for their own health that they are not willing to take.
3
12
168
Inadvertently I think Dr Kim may have become a standard bearer for humility, reflection and grace. If only all researchers behaved with such honour.
3
32
173
Hi Abby. Just wondering how we can break down barriers between ED and inpatient teams: to work more collaboratively and less in silos; to understand each other and walk in each other’s shoes occasionally. Surely that would not only help staff but patients too? Best wishes. Iain
7
9
168
Just a gentle reminder that the answer to A&Es/EDs being busy is not to cancel planned teaching sessions. Value and look after your staff and they will give back tenfold.
And if you do cancel these sessions don’t then say you care about ‘wellbeing’

5
48
167
There are so many good people in the world of Emergency Medicine. It’s a specialty of endless learning where you can do genuine good on a day to day basis. There is huge pressure on EDs at the moment and we must support each other with as much energy as we can muster.
3
27
166
This is the key to
#wellbeing
I believe. People don’t need fancy schemes, just decent working conditions, the ability to take leave when they’d like and a rewarding work environment for a fair salary. Spend the money (and time) on HR support, not chocolate.

Great line from an audience member in the session on resilience ‘I want my rota in good time, not a yoga mat’ 🤔
#rcpeSolutions
1
28
153
5
40
159
I am almost 50. I find Instagram influencers (particularly medical students telling me about their day) very confusing.
20
5
157
There really is something genuinely luxurious about getting into bed after a night shift. Have a good day you light loving losers.
8
3
157
Let’s be clear- this is association and not causation. When there aren’t strikes most A&Es across the UK are on the verge of a critical incident. The responsibility for this lies squarely at the door of those running the
#NHS
not the staff.

BREAKING: A critical incident has been declared at Nottinghamshire hospitals due to sustained pressure on the NHS and reduced staff because of the junior doctors strike
📺 Sky 501, Virgin 602, Freeview 233 and YouTube
118
87
235
6
42
159
Ok, Simon Carley has 25k followers and educates on a platform of Emergency Medicine. I have 7K followers and I’m really jealous.
Can we make my ‘voice’ as loud as his on Twitter?
Follow and RT me. Let’s do this 👍
PS. I know he is a Professor and all that, but I’m really needy
24
22
154
Hello again Abby. You have so many questions! Right now I’m wondering if the patient with atypical chest pain really did need a CTPA and an Echo, You really can’t be too careful. Or maybe you can. Oh gosh. It’s tricky.... Take care. Iain.
2
10
156


Our health system is being killed by the ‘just in case’ attendances followed by ‘just in case’ over investigation, the latter fuelled by a fear of criticism and reprimand.
5
18
154
As a doctor in an A&E I keep myself sane by focussing on caring first for those who really need it and I’m afraid the rest may need to wait. But I don’t feel guilty about that: that’s just the system we all work in.
Fundamental change is needed. But who is brave enough to do it?
10
12
151
This will come as absolutely no surprise to anyone working in emergency care. A few thoughts on why things have changed so much over the last decade (and why ‘attendance numbers’ are not comparable). 🧵

BREAKING: A&E four hours performance was 74.2% in March - missing NHSE's 76% target
8
26
24
7
45
149
Seriously? Where are they hoping they'll work? The 1970s? Are we not in more enlightened times?
@HSJEditor

41
106
139
I realise this may be rather controversial, but is it time we update the expected clinical examination for medical students to reflect real life? Palpating an apex beat for example. Has this ever really changed a single diagnostic decision? There’s plenty more of these examples…
20
3
145
“You’ve got this. If you need any help look at me”.
Surprising how much medical educators can learn from
@GlastoFest
Remember this next time you’re in Resus with a less experienced colleague and they too can be like
#Alex

Alex you absolute legend 👏
This kid just smashed
@Santandave1
x
@ajtracey
’s ‘Thiago Silva’ live at
#Glastonbury2019
#BBCGlasto
🔥🔥🔥🔥🔥
4K
65K
229K
2
40
142